

Direct-Acting Antiviral Prophylaxis in Kidney Transplantation From Hepatitis C Virus-Infected Donors to Noninfected Recipients: An Open-Label Nonrandomized Trial
- PMID: 29507971
- PMCID: PMC6108432
- DOI: 10.7326/M17-2871
Direct-Acting Antiviral Prophylaxis in Kidney Transplantation From Hepatitis C Virus-Infected Donors to Noninfected Recipients: An Open-Label Nonrandomized Trial
Abstract
Background: Given the high mortality rate for patients with end-stage kidney disease receiving dialysis and the efficacy and safety of hepatitis C virus (HCV) treatments, discarded kidneys from HCV-infected donors may be a neglected public health resource.
Objective: To determine the tolerability and feasibility of using direct-acting antivirals (DAAs) as prophylaxis before and after kidney transplantation from HCV-infected donors to non-HCV-infected recipients (that is, HCV D+/R- transplantation).
Design: Open-label nonrandomized trial. (ClinicalTrials.gov: NCT02781649).
Setting: Single center.
Participants: 10 HCV D+/R- kidney transplant candidates older than 50 years with no available living donors.
Intervention: Transplantation of kidneys from deceased donors aged 13 to 50 years with positive HCV RNA and HCV antibody test results. All recipients received a dose of grazoprevir (GZR), 100 mg, and elbasvir (EBR), 50 mg, immediately before transplantation. Recipients of kidneys from donors with genotype 1 infection continued receiving GZR-EBR for 12 weeks after transplantation; those receiving organs from donors with genotype 2 or 3 infection had sofosbuvir, 400 mg, added to GZR-EBR for 12 weeks of triple therapy.
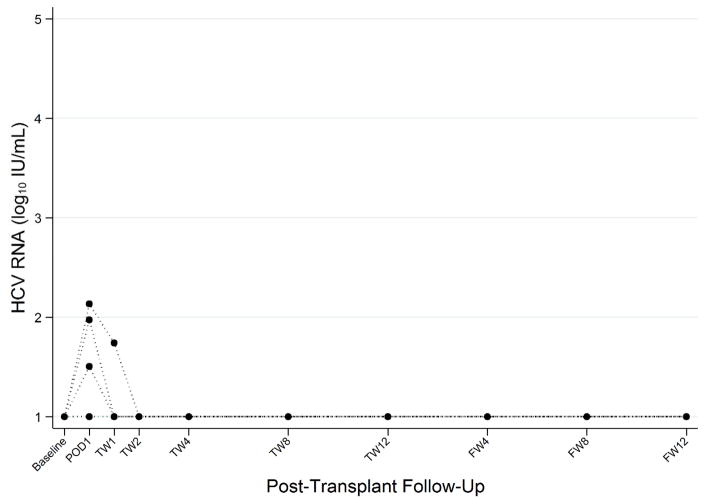
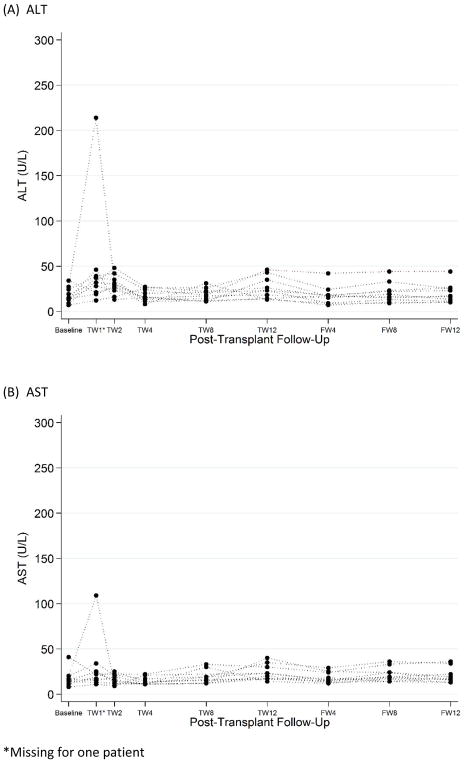
Measurements: The primary safety outcome was the incidence of adverse events related to GZR-EBR treatment. The primary efficacy outcome was the proportion of recipients with an HCV RNA level below the lower limit of quantification 12 weeks after prophylaxis.
Results: Among 10 HCV D+/R- transplant recipients, no treatment-related adverse events occurred, and HCV RNA was not detected in any recipient 12 weeks after treatment.
Limitation: Nonrandomized study design and a small number of patients.
Conclusion: Pre- and posttransplantation HCV treatment was safe and prevented chronic HCV infection in HCV D+/R- kidney transplant recipients. If confirmed in larger studies, this strategy should markedly expand organ options and reduce mortality for kidney transplant candidates without HCV infection.
Primary funding source: Merck Sharp & Dohme.
Conflict of interest statement
C. Durand has received research grants from Bristol Meyers Squibb, Gilead Sciences Merck Pharmaceuticals, and Viiv Healthcare, and has served as a scientific advisor for Bristol Meyers Squibb, Gilead Sciences, and Merck Pharmaceuticals. J. Sugarman serves on Merck KGaA’s Bioethics Advisory Panel and Stem Cell Research Oversight Committee; and Quintile’s Ethics Advisory Panel. M. Sulkowski served as scientific advisor for AbbVie, Gilead Sciences, Cocrystal, Janssen, Merck Pharmaceuticals, Trek and also received research grants from AbbVie, Gilead Sciences, and Merck Pharmaceuticals. N. Desai has served as a scientific advisor for Merck Pharmaceuticals.
Figures
References
-
- Wolfe RA, Ashby VB, Milford EL, Ojo AO, Ettenger RE, Agodoa LY, et al. Comparison of mortality in all patients on dialysis, patients on dialysis awaiting transplantation, and recipients of a first cadaveric transplant. N Engl J Med. 1999;341(23):1725–30. - PubMed
-
- Merion RM, Ashby VB, Wolfe RA, Distant DA, Hulbert-Shearon TE, Metzger RA, et al. Deceased-donor characteristics and the survival benefit of kidney transplantation. JAMA. 2005;294(21):2726–33. - PubMed
-
- Massie AB, Luo X, Chow EK, Alejo JL, Desai NM, Segev DL. Survival benefit of primary deceased donor transplantation with high-KDPI kidneys. Am J Transplant. 2014;14(10):2310–6. - PubMed
-
- Gill JS, Rose C, Pereira BJ, Tonelli M. The importance of transitions between dialysis and transplantation in the care of end-stage renal disease patients. Kidney Int. 2007;71(5):442–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical