

EADSG Guidelines: Insulin Therapy in Diabetes
- PMID: 29508275
- PMCID: PMC6104264
- DOI: 10.1007/s13300-018-0384-6
EADSG Guidelines: Insulin Therapy in Diabetes
Abstract
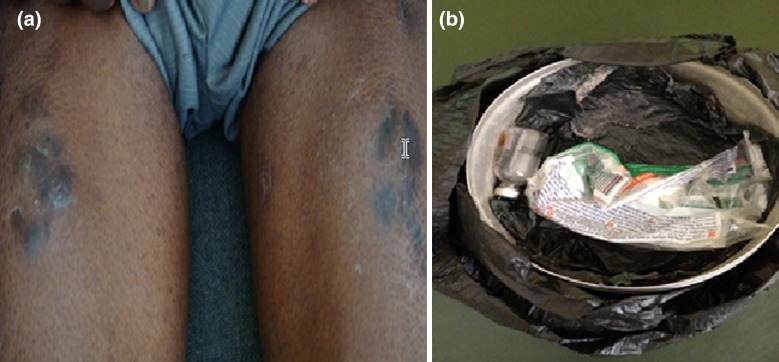
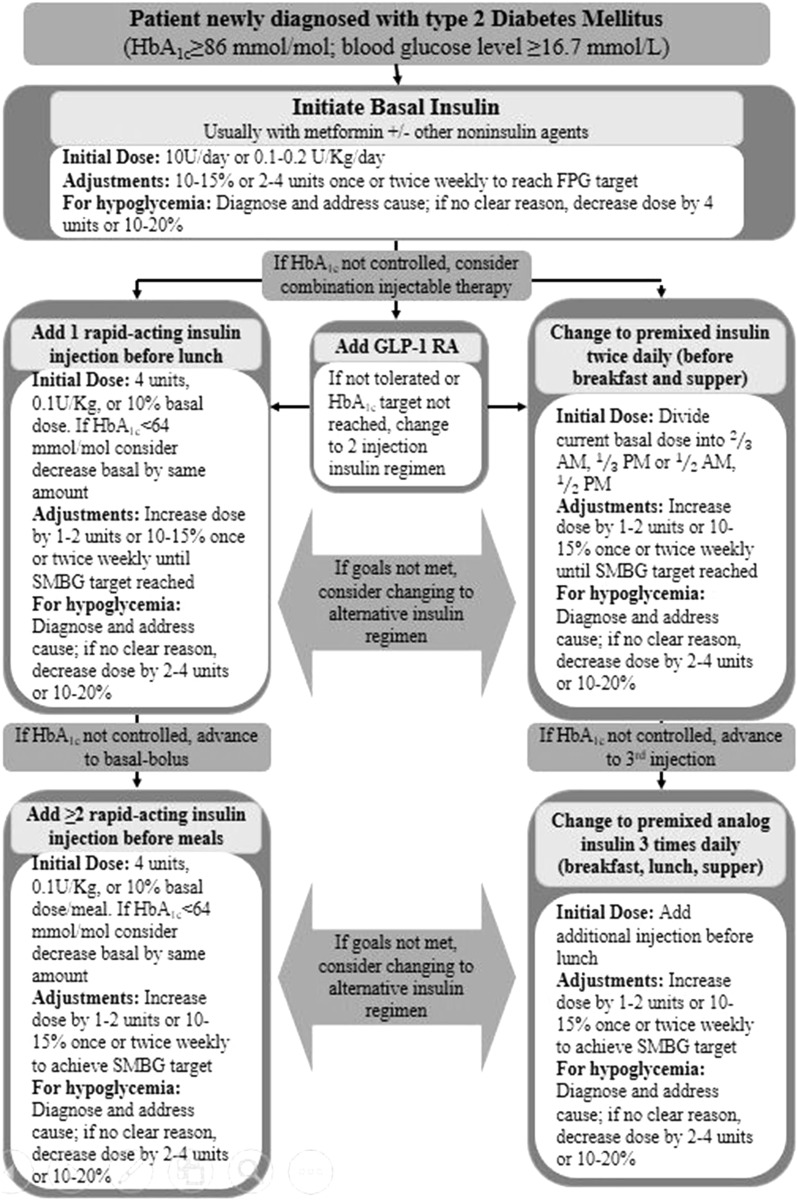
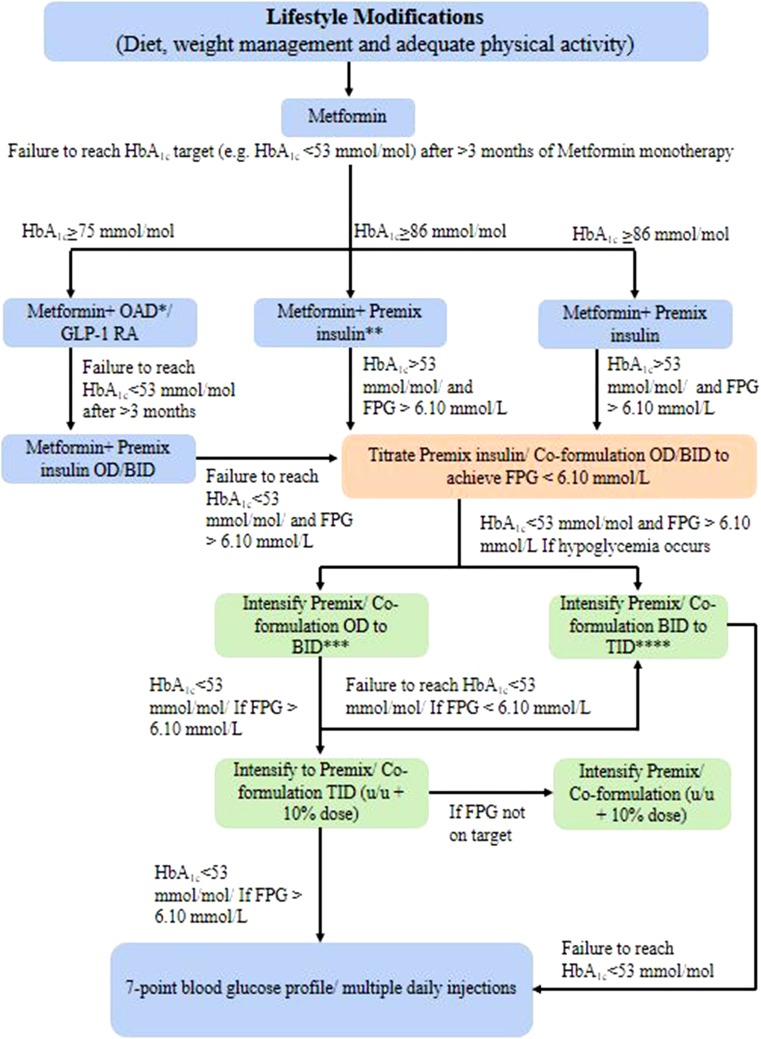
A diagnosis of diabetes or hyperglycemia should be confirmed prior to ordering, dispensing, or administering insulin (A). Insulin is the primary treatment in all patients with type 1 diabetes mellitus (T1DM) (A). Typically, patients with T1DM will require initiation with multiple daily injections at the time of diagnosis. This is usually short-acting insulin or rapid-acting insulin analogue given 0 to 15 min before meals together with one or more daily separate injections of intermediate or long-acting insulin. Two or three premixed insulin injections per day may be used (A). The target glycated hemoglobin A1c (HbA1c) for all children with T1DM, including preschool children, is recommended to be < 7.5% (< 58 mmol/mol). The target is chosen aiming at minimizing hyperglycemia, severe hypoglycemia, hypoglycemic unawareness, and reducing the likelihood of development of long-term complications (B). For patients prone to glycemic variability, glycemic control is best evaluated by a combination of results with self-monitoring of blood glucose (SMBG) (B). Indications for exogenous insulin therapy in patients with type 2 diabetes mellitus (T2DM) include acute illness or surgery, pregnancy, glucose toxicity, contraindications to or failure to achieve goals with oral antidiabetic medications, and a need for flexible therapy (B). In T2DM patients, with regards to achieving glycemic goals, insulin is considered alone or in combination with oral agents when HbA1c is ≥ 7.5% (≥ 58 mmol/mol); and is essential for treatment in those with HbA1c ≥ 10% (≥ 86 mmol/mol), when diet, physical activity, and other antihyperglycemic agents have been optimally used (B). The preferred method of insulin initiation in T2DM is to begin by adding a long-acting (basal) insulin or once-daily premixed/co-formulation insulin or twice-daily premixed insulin, alone or in combination with glucagon-like peptide-1 receptor agonist (GLP-1 RA) or in combination with other oral antidiabetic drugs (OADs) (B). If the desired glucose targets are not met, rapid-acting or short-acting (bolus or prandial) insulin can be added at mealtime to control the expected postprandial raise in glucose. An insulin regimen should be adopted and individualized but should, to the extent possible, closely resemble a natural physiologic state and avoid, to the extent possible, wide fluctuating glucose levels (C). Blood glucose monitoring is an integral part of effective insulin therapy and should not be omitted in the patient's care plan. Fasting plasma glucose (FPG) values should be used to titrate basal insulin, whereas both FPG and postprandial glucose (PPG) values should be used to titrate mealtime insulin (B). Metformin combined with insulin is associated with decreased weight gain, lower insulin dose, and less hypoglycemia when compared with insulin alone (C). Oral medications should not be abruptly discontinued when starting insulin therapy because of the risk of rebound hyperglycemia (D). Analogue insulin is as effective as human insulin but is associated with less postprandial hyperglycemia and delayed hypoglycemia (B). The shortest needles (currently the 4-mm pen and 6-mm syringe needles) are safe, effective, and less painful and should be the first-line choice in all patient categories; intramuscular (IM) injections should be avoided, especially with long-acting insulins, because severe hypoglycemia may result; lipohypertrophy is a frequent complication of therapy that distorts insulin absorption, and therefore, injections and infusions should not be given into these lesions and correct site rotation will help prevent them (A). Many patients in East Africa reuse syringes for various reasons, including financial. This is not recommended by the manufacturer and there is an association between needle reuse and lipohypertrophy. However, patients who reuse needles should not be subjected to alarming claims of excessive morbidity from this practice (A). Health care authorities and planners should be alerted to the risks associated with syringe or pen needles 6 mm or longer in children (A).
Keywords: Diabetes mellitus; East Africa; Guidelines; Hyperglycemia; Hypoglycemia; Insulin therapy; Type 1 diabetes mellitus (T1DM); Type 2 diabetes mellitus (T2DM).
Figures

Similar articles
-
Humalog Mix 25 in patients with type 2 diabetes which do not achieve acceptable glycemic control with oral agents: results from a phase III, randomized, parallel study.Rom J Intern Med. 2003;41(2):153-62. Rom J Intern Med. 2003. PMID: 15526500 Clinical Trial.
-
EMS Diabetic Protocols For Treat and Release.2023 Jul 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2023 Jul 17. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 32809447 Free Books & Documents.
-
Short-term intensive insulin therapy could be the preferred option for new onset Type 2 diabetes mellitus patients with HbA1c > 9.J Diabetes. 2017 Oct;9(10):890-893. doi: 10.1111/1753-0407.12581. Epub 2017 Aug 22. J Diabetes. 2017. PMID: 28661564
-
The importance of postprandial glycemic control: optimizing add-on therapy to basal insulin.Postgrad Med. 2016 Jan;128(1):137-44. doi: 10.1080/00325481.2016.1103640. Epub 2015 Nov 7. Postgrad Med. 2016. PMID: 26548422 Review.
-
Repaglinide : a pharmacoeconomic review of its use in type 2 diabetes mellitus.Pharmacoeconomics. 2004;22(6):389-411. doi: 10.2165/00019053-200422060-00005. Pharmacoeconomics. 2004. PMID: 15099124 Review.
Cited by
-
A critical review on diabetes mellitus type 1 and type 2 management approaches: from lifestyle modification to current and novel targets and therapeutic agents.Front Endocrinol (Lausanne). 2024 Oct 18;15:1440456. doi: 10.3389/fendo.2024.1440456. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 39493778 Free PMC article. Review.
-
Effectiveness of dapagliflozin as an insulin adjunct in type 1 diabetes: a semi-mechanistic exposure-response model.Front Pharmacol. 2023 Oct 25;14:1229255. doi: 10.3389/fphar.2023.1229255. eCollection 2023. Front Pharmacol. 2023. PMID: 37954838 Free PMC article.
-
Circulating serum fibroblast growth factor 21 as risk and prognostic biomarker of retinal artery occlusion.Sci Rep. 2024 May 24;14(1):11854. doi: 10.1038/s41598-024-62588-w. Sci Rep. 2024. PMID: 38789571 Free PMC article.
-
African Cuisine-Centered Insulin Therapy: Expert Opinion on the Management of Hyperglycaemia in Adult Patients with Type 2 Diabetes Mellitus.Diabetes Ther. 2021 Jan;12(1):37-54. doi: 10.1007/s13300-020-00958-z. Epub 2020 Nov 9. Diabetes Ther. 2021. PMID: 33169346 Free PMC article. Review.
-
Fixed-ratio Combinations (basal Insulin Plus GLP-1RA) In Type 2 Diabetes. an Analytical Review Of Pivotal Clinical Trials.Rev Diabet Stud. 2023 Mar 31;19(1):14-27. doi: 10.1900/RDS.2023.19.14. Rev Diabet Stud. 2023. PMID: 37185053 Free PMC article. Review.
References
-
- International Diabetes Federation. Diabetes atlas—8th edition. http://www.diabetesatlas.org/resources/2017-atlas.html. Accessed Dec 19, 2017. - PubMed
-
- Institute for Health Metrics and Evaluation Human Development Network. The World Bank. The global burden of disease: generating evidence, guiding policy—Sub-Saharan Africa Regional Edition. Seattle: IHME; 2013.
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
