

Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: a prospective cohort study
- PMID: 29508705
- PMCID: PMC6709878
- DOI: 10.1016/S2213-2600(18)30062-6
Clinical phenotypes of delirium during critical illness and severity of subsequent long-term cognitive impairment: a prospective cohort study
Abstract
Background: Delirium during critical illness results from numerous insults, which might be interconnected and yet individually contribute to long-term cognitive impairment. We sought to describe the prevalence and duration of clinical phenotypes of delirium (ie, phenotypes defined by clinical risk factors) and to understand associations between these clinical phenotypes and severity of subsequent long-term cognitive impairment.
Methods: In this multicentre, prospective cohort study, we included adult (≥18 years) medical or surgical ICU patients with respiratory failure, shock, or both as part of two parallel studies: the Bringing to Light the Risk Factors and Incidence of Neuropsychological Dysfunction in ICU Survivors (BRAIN-ICU) study, and the Delirium and Dementia in Veterans Surviving ICU Care (MIND-ICU) study. We assessed patients at least once a day for delirium using the Confusion Assessment Method-ICU and identified a priori-defined, non-mutually exclusive phenotypes of delirium per the presence of hypoxia, sepsis, sedative exposure, or metabolic (eg, renal or hepatic) dysfunction. We considered delirium in the absence of hypoxia, sepsis, sedation, and metabolic dysfunction to be unclassified. 3 and 12 months after discharge, we assessed cognition with the Repeatable Battery for the Assessment of Neuropsychological Status (RBANS). We used multiple linear regression to separately analyse associations between the duration of each phenotype of delirium and RBANS global cognition scores at 3-month and 12-month follow-up, adjusting for potential confounders.
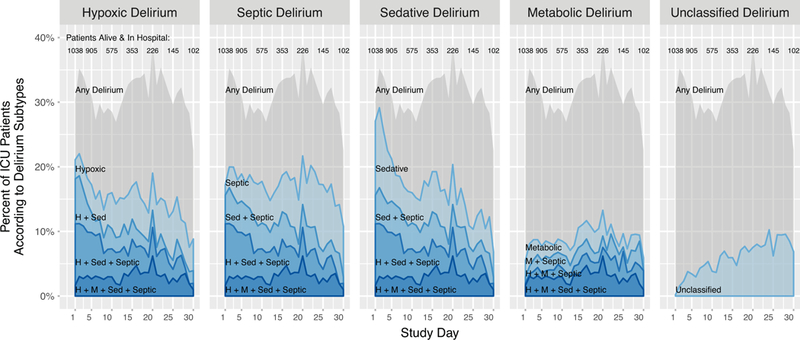
Findings: Between March 14, 2007, and May 27, 2010, 1048 participants were enrolled, eight of whom could not be analysed. Of 1040 participants, 708 survived to 3 months of follow-up and 628 to 12 months. Delirium was common, affecting 740 (71%) of 1040 participants at some point during the study and occurring on 4187 (31%) of all 13 434 participant-days. A single delirium phenotype was present on only 1355 (32%) of all 4187 participant-delirium days, whereas two or more phenotypes were present during 2832 (68%) delirium days. Sedative-associated delirium was most common (present during 2634 [63%] delirium days), and a longer duration of sedative-associated delirium predicted a worse RBANS global cognition score 12 months later, after adjusting for covariates (difference in score comparing 3 days vs 0 days: -4·03, 95% CI -7·80 to -0·26). Similarly, longer durations of hypoxic delirium (-3·76, 95% CI -7·16 to -0·37), septic delirium (-3·67, -7·13 to -0·22), and unclassified delirium (-4·70, -7·16 to -2·25) also predicted worse cognitive function at 12 months, whereas duration of metabolic delirium did not (1·14, -0·12 to 3·01).
Interpretation: Our findings suggest that clinicians should consider sedative-associated, hypoxic, and septic delirium, which often co-occur, as distinct indicators of acute brain injury and seek to identify all potential risk factors that may impact on long-term cognitive impairment, especially those that are iatrogenic and potentially modifiable such as sedation.
Funding: National Institutes of Health and the Department of Veterans Affairs.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures

Comment in
-
Does sedation related delirium matter?Lancet Respir Med. 2018 Mar;6(3):167-168. doi: 10.1016/S2213-2600(18)30067-5. Lancet Respir Med. 2018. PMID: 29508701 No abstract available.
References
-
- Ely EW, Shintani A, Truman B, et al. Delirium as a predictor of mortality in mechanically ventilated patients in the intensive care unit. JAMA 2004; 291(14): 1753–62. - PubMed
-
- Shehabi Y, Riker RR, Bokesch PM, Wisemandle W, Shintani A, Ely EW. Delirium duration and mortality in lightly sedated, mechanically ventilated intensive care patients. Crit Care Med 2010; 38(12): 2311–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
