

De novo donor-specific antibodies in belatacept-treated vs cyclosporine-treated kidney-transplant recipients: Post hoc analyses of the randomized phase III BENEFIT and BENEFIT-EXT studies
- PMID: 29509295
- PMCID: PMC6055714
- DOI: 10.1111/ajt.14721
De novo donor-specific antibodies in belatacept-treated vs cyclosporine-treated kidney-transplant recipients: Post hoc analyses of the randomized phase III BENEFIT and BENEFIT-EXT studies
Abstract
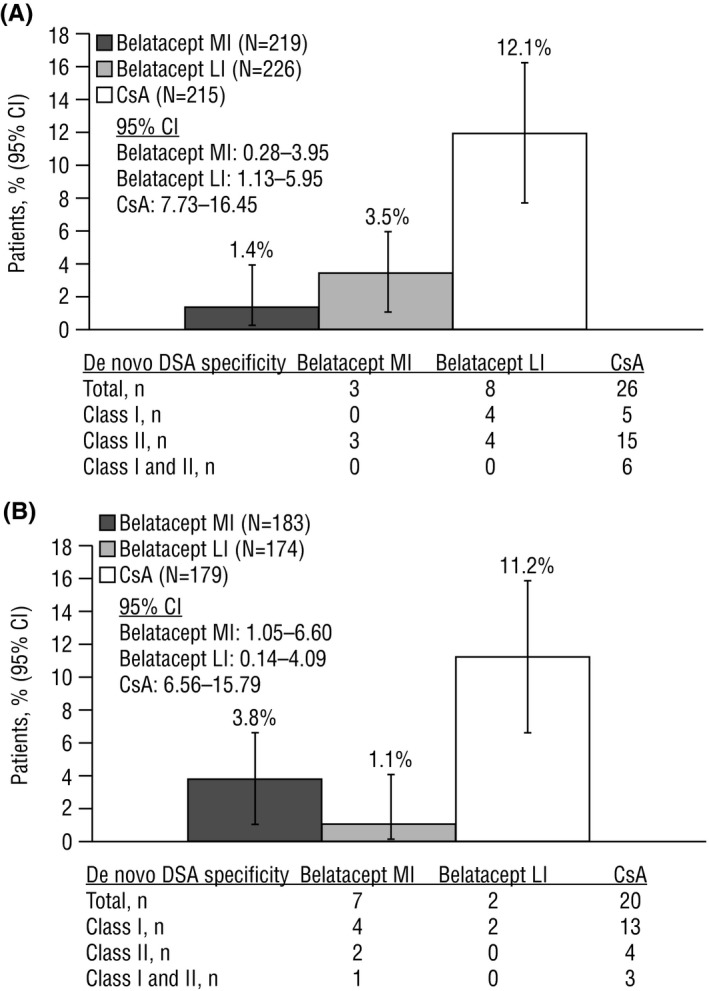
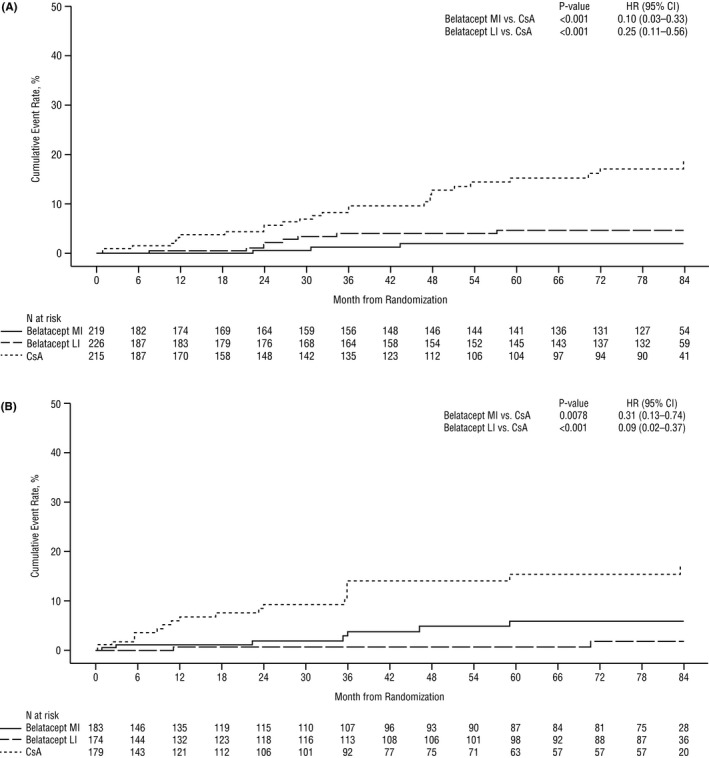
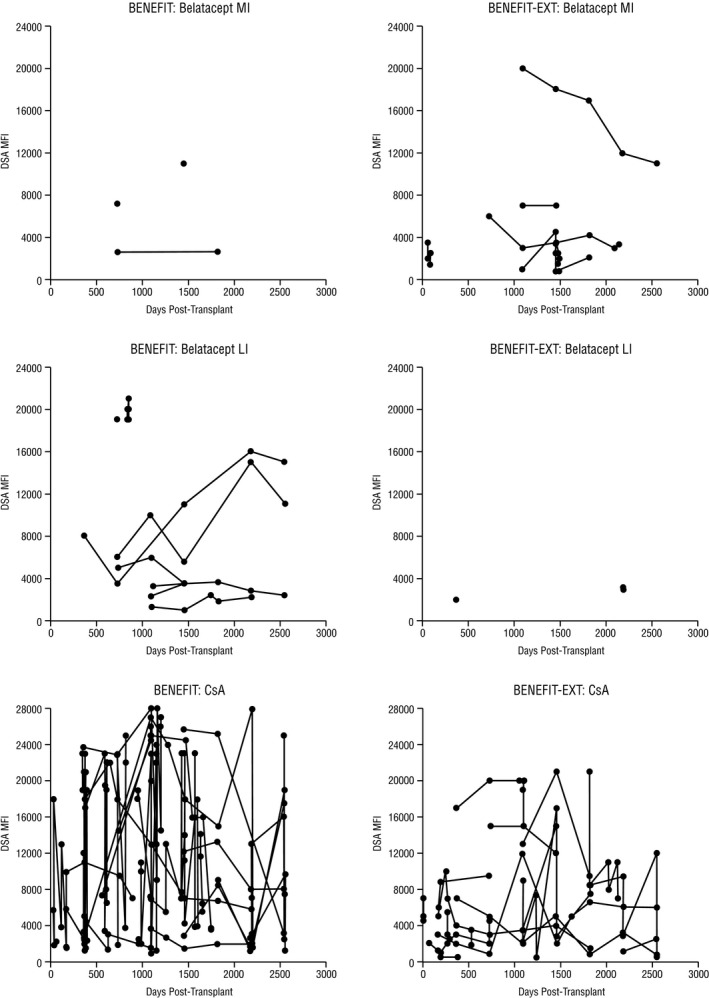
Donor-specific antibodies (DSAs) are associated with an increased risk of antibody-mediated rejection and graft failure. In BENEFIT and BENEFIT-EXT, kidney-transplant recipients were randomized to receive belatacept more intense (MI)-based, belatacept less intense (LI)-based, or cyclosporine-based immunosuppression for up to 7 years (84 months). The presence/absence of HLA-specific antibodies was determined at baseline, at months 6, 12, 24, 36, 48, 60, and 84, and at the time of clinically suspected episodes of acute rejection, using solid-phase flow-cytometry screening. Samples from anti-HLA-positive patients were further tested with a single-antigen bead assay to determine antibody specificities, presence/absence of DSAs, and mean fluorescence intensity (MFI) of any DSAs present. In BENEFIT, de novo DSAs developed in 1.4%, 3.5%, and 12.1% of belatacept MI-treated, belatacept LI-treated, and cyclosporine-treated patients, respectively. The corresponding values in BENEFIT-EXT were 3.8%, 1.1%, and 11.2%. Per Kaplan-Meier analysis, de novo DSA incidence was significantly lower in belatacept-treated vs cyclosporine-treated patients over 7 years in both studies (P < .01). In patients who developed de novo DSAs, belatacept-based immunosuppression was associated with numerically lower MFI vs cyclosporine-based immunosuppression. Although derived post hoc, these data suggest that belatacept-based immunosuppression suppresses de novo DSA development more effectively than cyclosporine-based immunosuppression.
Keywords: antibody biology; belatacept; clinical research/practice; clinical trial; cyclosporin A (CsA); immunosuppressant - calcineurin inhibitor; immunosuppressant - fusion proteins and monoclonal antibodies; kidney transplantation/nephrology.
© 2018 The Authors. American Journal of Transplantation published by Wiley Periodicals, Inc. on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
-
- Squibb Bristol‐Myers . Belatacept (NULOJIX) Prescribing Information. Princeton, NJ: Bristol‐Myers Squibb Company; 2016.
-
- Vincenti F, Charpentier B, Vanrenterghem Y, et al. A phase III study of belatacept‐based immunosuppression regimens vs cyclosporine in renal transplant recipients (BENEFIT study). Am J Transplant. 2010;10:535‐546. - PubMed
-
- Durrbach A, Pestana JM, Pearson T, et al. A phase III study of belatacept vs cyclosporine in kidney transplants from extended criteria donors (BENEFIT‐EXT study). Am J Transplant. 2010;10:547‐557. - PubMed
-
- Vincenti F, Rostaing L, Grinyo J, et al. Belatacept and long‐term outcomes in kidney transplantation. N Engl J Med. 2016;374:333‐343. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
