

Patterns and temporal trends of comorbidity among adult patients with incident cardiovascular disease in the UK between 2000 and 2014: A population-based cohort study
- PMID: 29509757
- PMCID: PMC5839540
- DOI: 10.1371/journal.pmed.1002513
Patterns and temporal trends of comorbidity among adult patients with incident cardiovascular disease in the UK between 2000 and 2014: A population-based cohort study
Abstract
Background: Multimorbidity in people with cardiovascular disease (CVD) is common, but large-scale contemporary reports of patterns and trends in patients with incident CVD are limited. We investigated the burden of comorbidities in patients with incident CVD, how it changed between 2000 and 2014, and how it varied by age, sex, and socioeconomic status (SES).
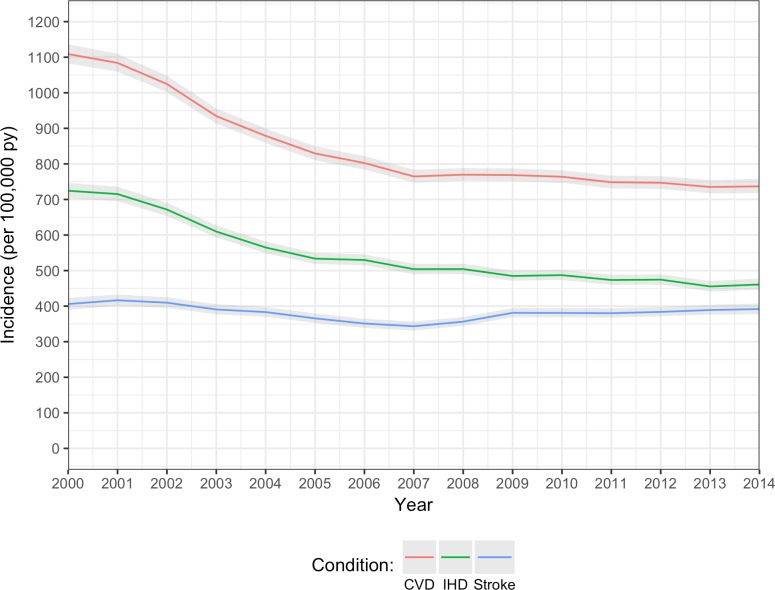
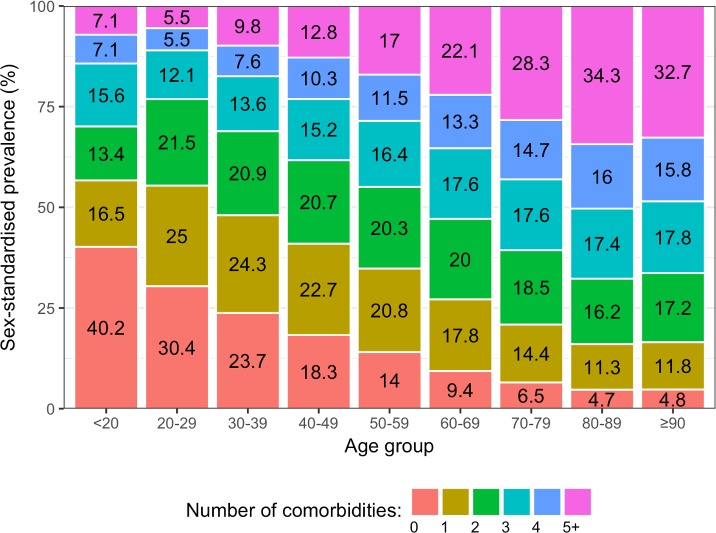
Methods and findings: We used the UK Clinical Practice Research Datalink with linkage to Hospital Episode Statistics, a population-based dataset from 674 UK general practices covering approximately 7% of the current UK population. We estimated crude and age/sex-standardised (to the 2013 European Standard Population) prevalence and 95% confidence intervals for 56 major comorbidities in individuals with incident non-fatal CVD. We further assessed temporal trends and patterns by age, sex, and SES groups, between 2000 and 2014. Among a total of 4,198,039 people aged 16 to 113 years, 229,205 incident cases of non-fatal CVD, defined as first diagnosis of ischaemic heart disease, stroke, or transient ischaemic attack, were identified. Although the age/sex-standardised incidence of CVD decreased by 34% between 2000 to 2014, the proportion of CVD patients with higher numbers of comorbidities increased. The prevalence of having 5 or more comorbidities increased 4-fold, rising from 6.3% (95% CI 5.6%-17.0%) in 2000 to 24.3% (22.1%-34.8%) in 2014 in age/sex-standardised models. The most common comorbidities in age/sex-standardised models were hypertension (28.9% [95% CI 27.7%-31.4%]), depression (23.0% [21.3%-26.0%]), arthritis (20.9% [19.5%-23.5%]), asthma (17.7% [15.8%-20.8%]), and anxiety (15.0% [13.7%-17.6%]). Cardiometabolic conditions and arthritis were highly prevalent among patients aged over 40 years, and mental illnesses were highly prevalent in patients aged 30-59 years. The age-standardised prevalence of having 5 or more comorbidities was 19.1% (95% CI 17.2%-22.7%) in women and 12.5% (12.0%-13.9%) in men, and women had twice the age-standardised prevalence of depression (31.1% [28.3%-35.5%] versus 15.0% [14.3%-16.5%]) and anxiety (19.6% [17.6%-23.3%] versus 10.4% [9.8%-11.8%]). The prevalence of depression was 46% higher in the most deprived fifth of SES compared with the least deprived fifth (age/sex-standardised prevalence of 38.4% [31.2%-62.0%] versus 26.3% [23.1%-34.5%], respectively). This is a descriptive study of routine electronic health records in the UK, which might underestimate the true prevalence of diseases.
Conclusions: The burden of multimorbidity and comorbidity in patients with incident non-fatal CVD increased between 2000 and 2014. On average, older patients, women, and socioeconomically deprived groups had higher numbers of comorbidities, but the type of comorbidities varied by age and sex. Cardiometabolic conditions contributed substantially to the burden, but 4 out of the 10 top comorbidities were non-cardiometabolic. The current single-disease paradigm in CVD management needs to broaden and incorporate the large and increasing burden of comorbidities.
Conflict of interest statement
KR receives a stipend as a specialty consulting editor for PLOS Medicine and serves on the journal's editorial board. KR also served as a guest editor on PLOS Medicine’s Cardiovascular Disease Special Issue.
Figures





References
-
- de Groot V, Beckerman H, Lankhorst GJ, Bouter LM. How to measure comorbidity. a critical review of available methods. J Clin Epidemiol. 2003;56(3):221–9. doi: 10.1016/S0895-4356(02)00585-1 - DOI - PubMed
-
- Glynn LG, Valderas JM, Healy P, Burke E, Newell J, Gillespie P. The prevalence of multimorbidity in primary care and its effect on health care utilization and cost. Fam Pract. 2011;28(5):516–23. doi: 10.1093/fampra/cmr013 - DOI - PubMed
-
- Palladino R. Associations between multimorbidity, healthcare utilisation and health status: evidence from 16 European countries. Age Ageing. 2016;45(3):431–5. doi: 10.1093/ageing/afw044 - DOI - PMC - PubMed
-
- Murray CJL, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–223. doi: 10.1016/S0140-6736(12)61689-4 - DOI - PubMed
-
- Diederichs C, Berger K, Bartels DB. The measurement of multiple chronic diseases—a systematic review on existing multimorbidity indices. J Gerontol A Biol Sci Med Sci. 2011;66(3):301–11. doi: 10.1093/gerona/glq208 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
