

Multimorbidity and survival for patients with acute myocardial infarction in England and Wales: Latent class analysis of a nationwide population-based cohort
- PMID: 29509764
- PMCID: PMC5839532
- DOI: 10.1371/journal.pmed.1002501
Multimorbidity and survival for patients with acute myocardial infarction in England and Wales: Latent class analysis of a nationwide population-based cohort
Abstract
Background: There is limited knowledge of the scale and impact of multimorbidity for patients who have had an acute myocardial infarction (AMI). Therefore, this study aimed to determine the extent to which multimorbidity is associated with long-term survival following AMI.
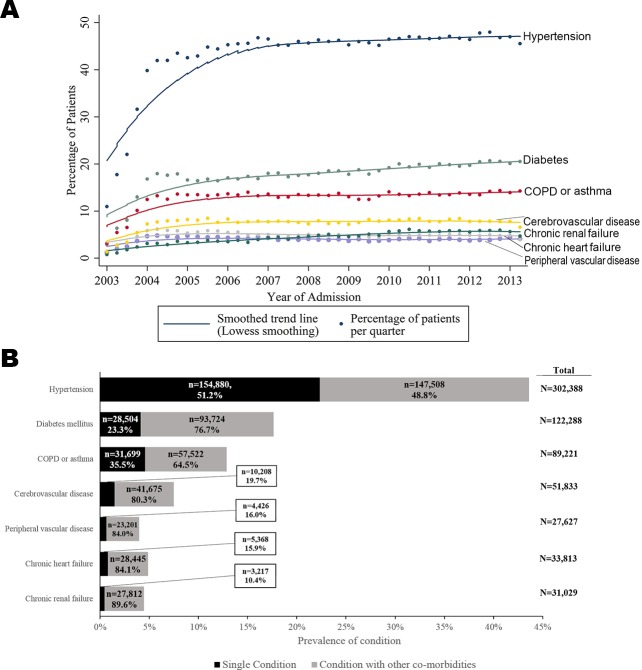
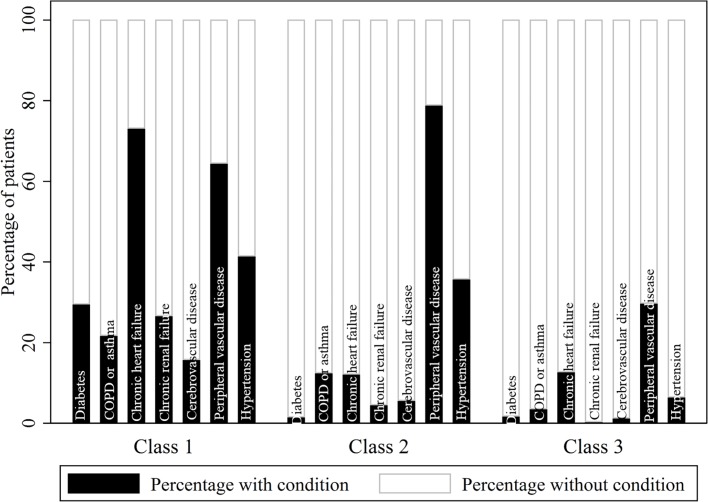
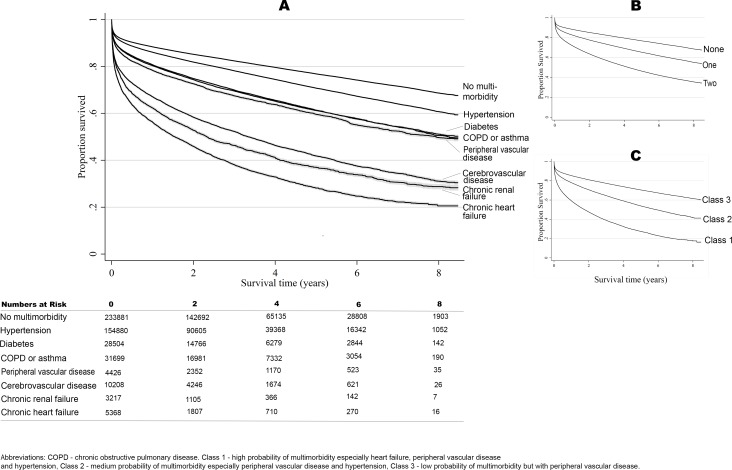
Methods and findings: This national observational study included 693,388 patients (median age 70.7 years, 452,896 [65.5%] male) from the Myocardial Ischaemia National Audit Project (England and Wales) who were admitted with AMI between 1 January 2003 and 30 June 2013. There were 412,809 (59.5%) patients with multimorbidity at the time of admission with AMI, i.e., having at least 1 of the following long-term health conditions: diabetes, chronic obstructive pulmonary disease or asthma, heart failure, renal failure, cerebrovascular disease, peripheral vascular disease, or hypertension. Those with heart failure, renal failure, or cerebrovascular disease had the worst outcomes (39.5 [95% CI 39.0-40.0], 38.2 [27.7-26.8], and 26.6 [25.2-26.4] deaths per 100 person-years, respectively). Latent class analysis revealed 3 multimorbidity phenotype clusters: (1) a high multimorbidity class, with concomitant heart failure, peripheral vascular disease, and hypertension, (2) a medium multimorbidity class, with peripheral vascular disease and hypertension, and (3) a low multimorbidity class. Patients in class 1 were less likely to receive pharmacological therapies compared with class 2 and 3 patients (including aspirin, 83.8% versus 87.3% and 87.2%, respectively; β-blockers, 74.0% versus 80.9% and 81.4%; and statins, 80.6% versus 85.9% and 85.2%). Flexible parametric survival modelling indicated that patients in class 1 and class 2 had a 2.4-fold (95% CI 2.3-2.5) and 1.5-fold (95% CI 1.4-1.5) increased risk of death and a loss in life expectancy of 2.89 and 1.52 years, respectively, compared with those in class 3 over the 8.4-year follow-up period. The study was limited to all-cause mortality due to the lack of available cause-specific mortality data. However, we isolated the disease-specific association with mortality by providing the loss in life expectancy following AMI according to multimorbidity phenotype cluster compared with the general age-, sex-, and year-matched population.
Conclusions: Multimorbidity among patients with AMI was common, and conferred an accumulative increased risk of death. Three multimorbidity phenotype clusters that were significantly associated with loss in life expectancy were identified and should be a concomitant treatment target to improve cardiovascular outcomes.
Trial registration: ClinicalTrials.gov NCT03037255.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests to disclose: CPG has received speaker and consulting honoraria from AstraZeneca and Novartis. KAAF reports grants and personal fees from AstraZeneca, personal fees from Sanofi/Regeneron, grants and personal fees from Bayer/Janssen, personal fees from GSK, grants and personal fees from Lilly outside of the submitted work. MAM reports unrestricted educational grants for Terumo, Daiichi Sankyo, and personal fees from AstraZeneca, Cordis outside of submitted work. TJ has received speaker and consulting honoraria from AstraZeneca, MSD and Aspen. HH is a National Institute for Health Research (NIHR) Senior Investigator (grant NF-SI-0616-10066) and is funded by awards from the Medical Research Council, Arthritis Research UK, British Heart Foundation, Cancer Research UK, Chief Scientist Office, Economic and Social Research Council, Engineering and Physical Sciences Research Council, NIHR, National Institute for Social Care and Health Research, and Wellcome Trust (grant MR/K006584/1).
Figures
References
-
- Barnett K, Mercer SW, Norbury M, Watt G, Wyke S, Guthrie B. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi: 10.1016/S0140-6736(12)60240-2 - DOI - PubMed
-
- World Health Organization. Global status report on noncommunicable diseases 2010: description of the global burden of NCDs, their risk factors and determinants Geneva: World Health Organization; 2011. [cited 2011 Dec 22]. Available from: http://www.who.int/nmh/publications/ncd_report2010/en/.
-
- Rashid M, Kwok CS, Gale CP, Doherty P, Olier I, Sperrin M, et al. Impact of co-morbid burden on mortality in patients with coronary heart disease, heart failure and cerebrovascular accident: a systematic review and meta-analysis. Eur Heart J Qual Care Clin Outcomes. 2017;3(1):20–36. doi: 10.1093/ehjqcco/qcw025 - DOI - PubMed
-
- Fox K, Steg P, Eagle K, Goodman S, Anderson F, Granger C, et al. Decline in rates of death and heart failure in acute coronary syndromes, 1999–2006. JAMA. 2007;297(17):1892–900. doi: 10.1001/jama.297.17.1892 - DOI - PubMed
-
- Alzuhairi K, Søgaard P, Ravkilde J, Gislason G, Køber L, Torp-Pedersen C. Incidence and outcome of first myocardial infarction according to gender and age in Denmark over a 35-year period (1978–2012). Eur Heart J Qual Care Clin Outcomes. 2015;1:72–8. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
