

Trajectories of functional decline in older adults with neuropsychiatric and cardiovascular multimorbidity: A Swedish cohort study
- PMID: 29509768
- PMCID: PMC5839531
- DOI: 10.1371/journal.pmed.1002503
Trajectories of functional decline in older adults with neuropsychiatric and cardiovascular multimorbidity: A Swedish cohort study
Abstract
Background: Functional decline is a strong health determinant in older adults, and chronic diseases play a major role in this age-related phenomenon. In this study, we explored possible clinical pathways underlying functional heterogeneity in older adults by quantifying the impact of cardiovascular (CV) and neuropsychiatric (NP) chronic diseases and their co-occurrence on trajectories of functional decline.
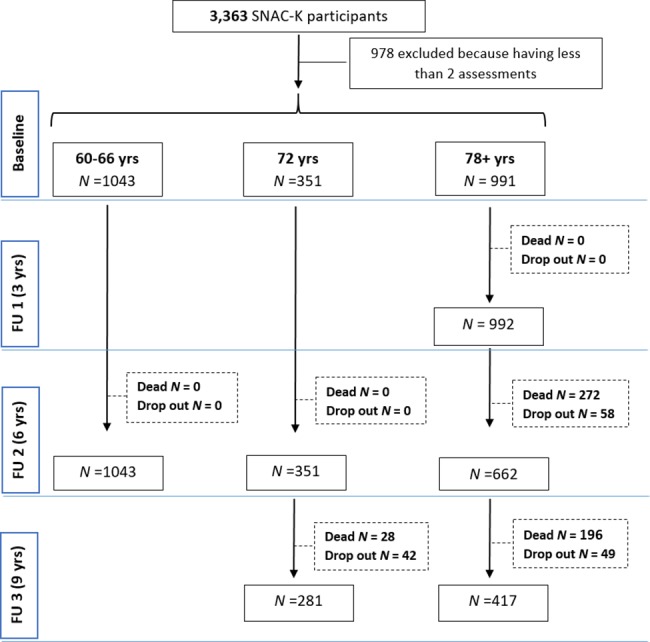
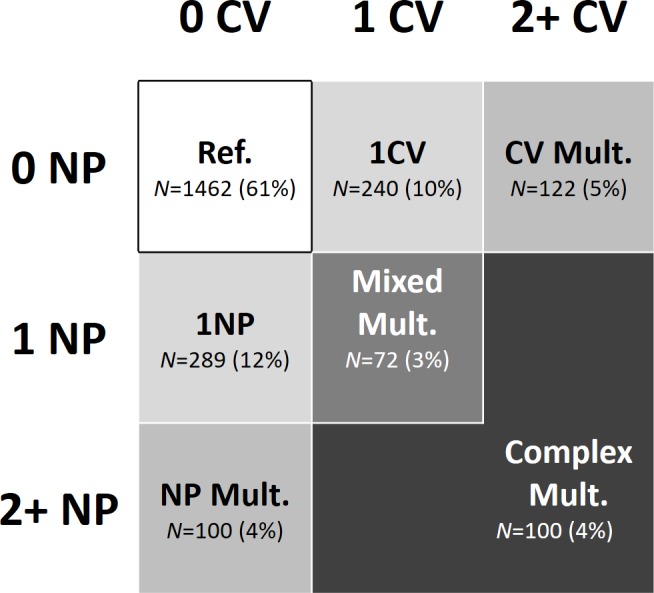
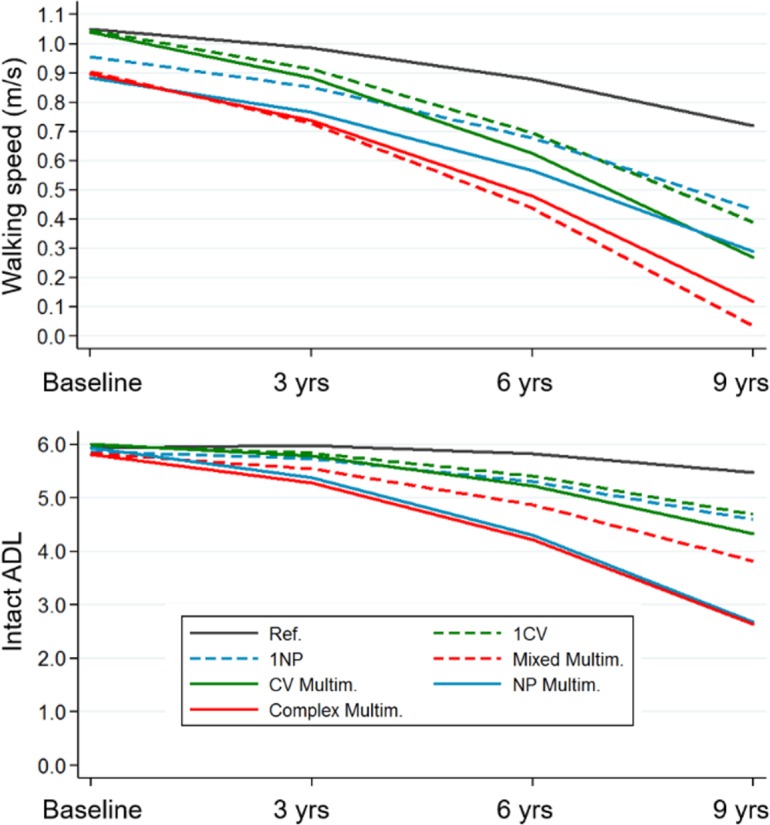
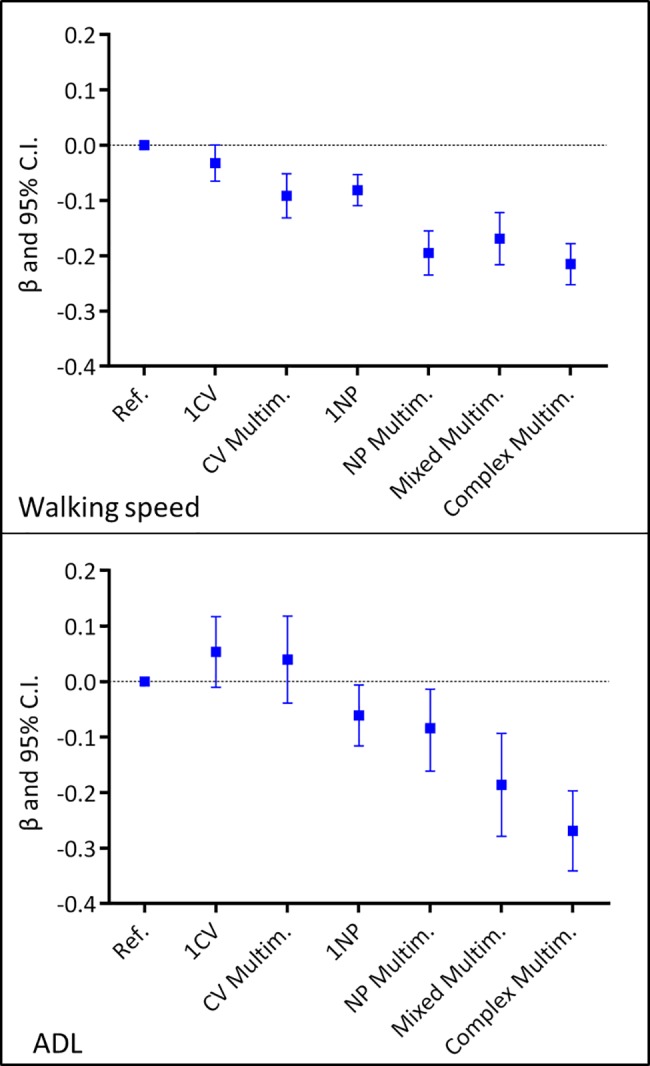
Methods and findings: We studied 2,385 people ≥60 years (range 60-101 years) participating in the Swedish National study of Aging and Care in Kungsholmen (SNAC-K). Participants underwent clinical examination at baseline (2001-2004) and every 3 or 6 years for up to 9 years. We grouped participants on the basis of 7 mutually exclusive clinical patterns of 0, 1, or more CV and NP diseases and their co-occurrence, from a group without any CV and NP disease to a group characterised by the presence of CV or NP multimorbidity, accompanied by at least 1 other CV or NP disorder. The group with no CV and/or NP diseases served as the reference group. Functional decline was estimated over 9 years of follow-up by measuring mobility (walking speed, m/s) and independence (ability to carry out six activities of daily living [ADL]). Mixed-effect linear regression models were used (1) to explore the individual-level prognostic predictivity of the different CV and NP clinical patterns at baseline and (2) to quantify the association between the clinical patterns and functional decline at the group level by entering the clinical patterns as time-varying measures. During the 9-year follow-up, participants with multiple CV and NP diseases had the steepest decline in walking speed (up to 0.7 m/s; p < 0.001) and ADL independence (up to three impairments in ADL, p < 0.001) (reference group: participants without any CV and NP disease). When the clinical patterns were analyzed as time varying, isolated CV multimorbidity impacted only walking speed (β -0.1; p < 0.001). Conversely, all the clinical patterns that included at least 1 NP disease were significantly associated with decline in both walking speed (β -0.21--0.08; p < 0.001) and ADL independence (β -0.27--0.06; p < 0.05). Groups with the most complex clinical patterns had 5%-20% lower functioning at follow-up than the reference group. Key limitations of the study include that we did not take into account the specific weight of single diseases and their severity and that the exclusion of participants with less than 2 assessments may have led to an underestimation of the tested associations.
Conclusions: In older adults, different patterns of CV and NP morbidity lead to different trajectories of functional decline over time, a finding that explains part of the heterogeneity observed in older adults' functionality. NP diseases, alone or in association, are prevalent and major determinants of functional decline, whereas isolated CV multimorbidity is associated only with declines in mobility.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K (2013) Frailty in elderly people. Lancet 381: 752–762. doi: 10.1016/S0140-6736(12)62167-9 - DOI - PMC - PubMed
-
- Newman AB, Sanders JL, Kizer JR, Boudreau RM, Odden MC, Zeki Al Hazzouri A, et al. (2016) Trajectories of function and biomarkers with age: the CHS All Stars Study. Int J Epidemiol 45: 1135–1145. doi: 10.1093/ije/dyw092 - DOI - PMC - PubMed
-
- Marengoni A, Angleman S, Meinow B, Santoni G, Mangialasche F, Rizzuto D, et al. (2016) Coexisting chronic conditions in the older population: Variation by health indicators. Eur J Intern Med 31: 29–34. doi: 10.1016/j.ejim.2016.02.014 - DOI - PubMed
-
- Marengoni A, Angleman S, Melis R, Mangialasche F, Karp A, Garmen A, et al. (2011) Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev 10: 430–439. doi: 10.1016/j.arr.2011.03.003 - DOI - PubMed
-
- Klimek P, Aichberger S, Thurner S (2016) Disentangling genetic and environmental risk factors for individual diseases from multiplex comorbidity networks. Sci Rep 6: 39658 doi: 10.1038/srep39658 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
