

Flow Preservation of Umbilical Vein for Autologous Shunt and Cardiovascular Reconstruction
- PMID: 29510094
- PMCID: PMC6292668
- DOI: 10.1016/j.athoracsur.2018.01.076
Flow Preservation of Umbilical Vein for Autologous Shunt and Cardiovascular Reconstruction
Abstract
Background: Synthetic graft materials are commonly used for shunts and cardiovascular reconstruction in neonates, but are prone to thrombosis and scarring. The umbilical vein is a potential source of autologous, endothelialized tissue for neonatal shunts and tissue reconstruction, but requires preservation before implantation.
Methods: Umbilical cords were collected in UW solution with antibiotics at 4°C until dissection. Umbilical vein segments were tested for burst pressure before and after 2 weeks of preservation. Umbilical veins segments were preserved under static or flow conditions at 4°C in UW solution with 5% human plasma lysate for 7 days. Veins were evaluated with histopathology, scanning electron microscopy, and platelet adhesion testing.
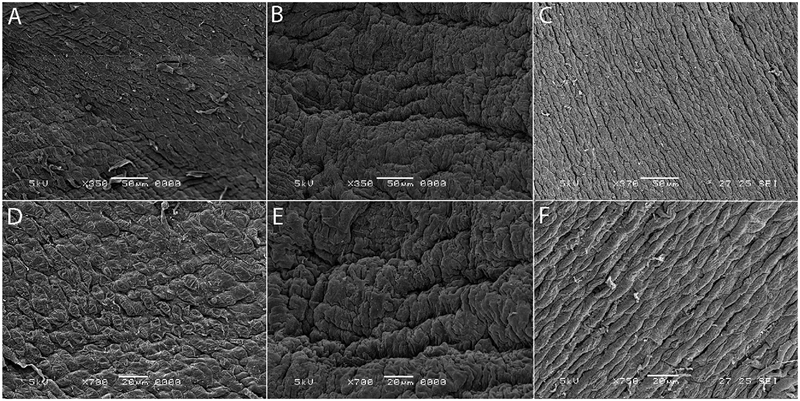
Results: Umbilical veins have no difference in burst pressure at harvest (n = 16) compared with 2 weeks of preservation (n = 11; 431 ± 229 versus 438 ± 244 mm Hg). After 1 week, static and flow-preserved veins showed viability of the vessel segments with endothelium staining positive for CD31, von Willebrand factor, and endothelial nitric oxide synthase. Scanning electron microscopy demonstrated preservation of normal endothelial morphology and flow alignment in the flow-preserved samples compared with cobblestone endothelial appearance and some endothelial cell loss in the static samples. Static samples had significantly more platelet adhesion than flow-preserved samples did.
Conclusions: Umbilical veins have adequate burst strength to function at neonatal systemic pressures. Preservation under flow conditions demonstrated normal endothelial and overall vascular morphology with less platelet adhesion compared with static samples. Preserved autologous umbilical veins are potential source for endothelialized shunts or cardiovascular repair tissue for neonates.
Copyright © 2018 The Society of Thoracic Surgeons. Published by Elsevier Inc. All rights reserved.
Figures






Similar articles
-
Morphology and function of dog arterial grafts preserved in UW-solution.Eur J Vasc Endovasc Surg. 1995 Nov;10(4):431-9. doi: 10.1016/s1078-5884(05)80165-0. Eur J Vasc Endovasc Surg. 1995. PMID: 7489211
-
Functional and morphological evaluation of canine veins following preservation in different storage media.J Surg Res. 1997 Mar;68(2):106-15. doi: 10.1006/jsre.1996.4981. J Surg Res. 1997. PMID: 9184668
-
Endothelial cell preservation at hypothermic to normothermic conditions using clinical and experimental organ preservation solutions.Exp Cell Res. 2013 Oct 15;319(17):2501-13. doi: 10.1016/j.yexcr.2013.05.011. Epub 2013 Jun 20. Exp Cell Res. 2013. PMID: 23792081
-
[Implantation of formalin-preserved umbilical veins as dialysis shunts--a new method of allogenic blood vessel graft (author's transl)].Thoraxchir Vask Chir. 1977 Dec;25(6):415-21. doi: 10.1055/s-0028-1097071. Thoraxchir Vask Chir. 1977. PMID: 601763 German.
-
Optimal techniques for harvesting and preparation of reversed autogenous vein grafts for use as arterial substitutes: a review.Surgery. 1984 Nov;96(5):886-94. Surgery. 1984. PMID: 6387991 Review.
Cited by
-
Regeneration of Vascular Endothelium in Different Large Vessels.Int J Mol Sci. 2025 Jan 20;26(2):837. doi: 10.3390/ijms26020837. Int J Mol Sci. 2025. PMID: 39859550 Free PMC article. Review.
-
Hemodynamics and Wall Mechanics of Vascular Graft Failure.Arterioscler Thromb Vasc Biol. 2024 May;44(5):1065-1085. doi: 10.1161/ATVBAHA.123.318239. Epub 2024 Apr 4. Arterioscler Thromb Vasc Biol. 2024. PMID: 38572650 Free PMC article. Review.
References
-
- Guzzetta NA, Foster GS, Mruthinti N, Kilgore PD, Miller BE, Kanter KR. In-hospital shunt occlusion in infants undergoing a modified blalock-taussig shunt. Ann Thorac Surg 2013;96: 176–82. - PubMed
-
- McKenzie ED, Khan MS, Samayoa AX, et al. The Blalock-Taussig shunt revisited: a contemporary experience. J Am Coll Surg 2013;216:699–704, discussion 704–6. - PubMed
-
- Petrucci O, O’Brien SM, Jacobs ML, Jacobs JP, Manning PB, Eghtesady P. Risk factors for mortality and morbidity after the neonatal Blalock-Taussig shunt procedure. Ann Thorac Surg 2011;92:642–51, discussion 651–2. - PubMed
-
- Kogon BE, Kanter K, Alsoufi B, Maher K, Oster ME. Outcomes and hospital costs associated with the Norwood operation: beyond morbidity and mortality—CORRIGENDUM. Cardiol Young 2015;25:860. - PubMed
-
- Wells WJ, Yu RJ, Batra AS, Monforte H, Sintek C, Starnes VA. Obstruction in modified Blalock shunts: a quantitative analysis with clinical correlation. Ann Thorac Surg 2005;79:2072–6. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
