

Time to Epinephrine Administration and Survival From Nonshockable Out-of-Hospital Cardiac Arrest Among Children and Adults
- PMID: 29511001
- PMCID: PMC5940513
- DOI: 10.1161/CIRCULATIONAHA.117.033067
Time to Epinephrine Administration and Survival From Nonshockable Out-of-Hospital Cardiac Arrest Among Children and Adults
Abstract
Background: Previous studies have demonstrated that earlier epinephrine administration is associated with improved survival from out-of-hospital cardiac arrest (OHCA) with shockable initial rhythms. However, the effect of epinephrine timing on patients with nonshockable initial rhythms is unclear. The objective of this study was to measure the association between time to epinephrine administration and survival in adults and children with emergency medical services (EMS)-treated OHCA with nonshockable initial rhythms.
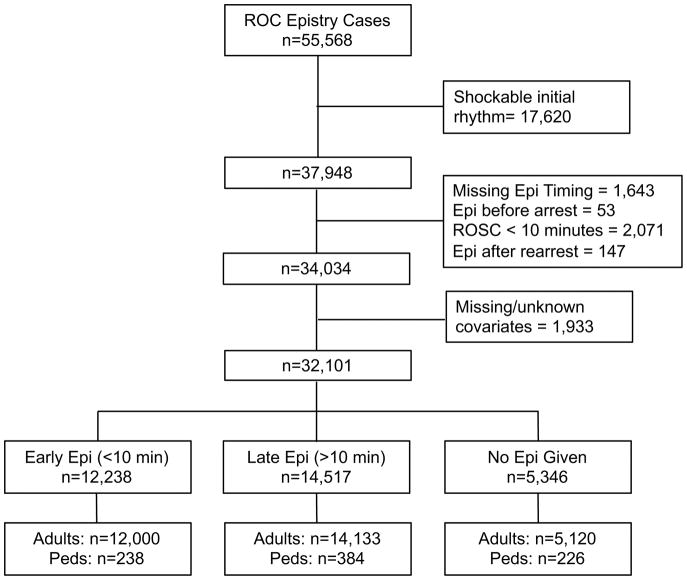
Methods: We performed a secondary analysis of OHCAs prospectively identified by the Resuscitation Outcomes Consortium network from June 4, 2011, to June 30, 2015. We included patients of all ages with an EMS-treated OHCA and an initial nonshockable rhythm. We excluded those with return of spontaneous circulation in <10 minutes. We conducted a subgroup analysis involving patients <18 years of age. The primary exposure was time (minutes) from arrival of the first EMS agency to the first dose of epinephrine. Secondary exposure was time to epinephrine dichotomized as early (<10 minutes) or late (≥10 minutes). The primary outcome was survival to hospital discharge. We adjusted for Utstein covariates and Resuscitation Outcomes Consortium study site.
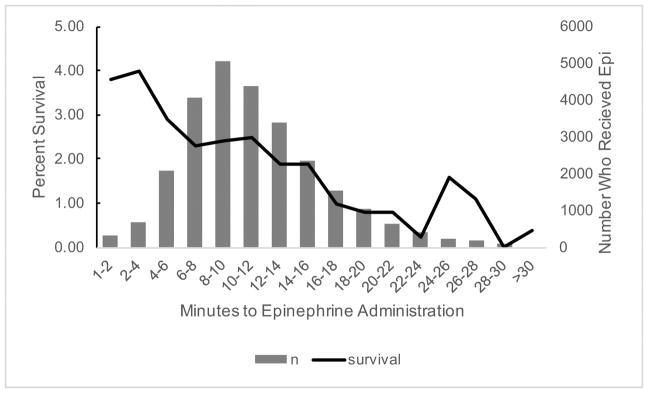
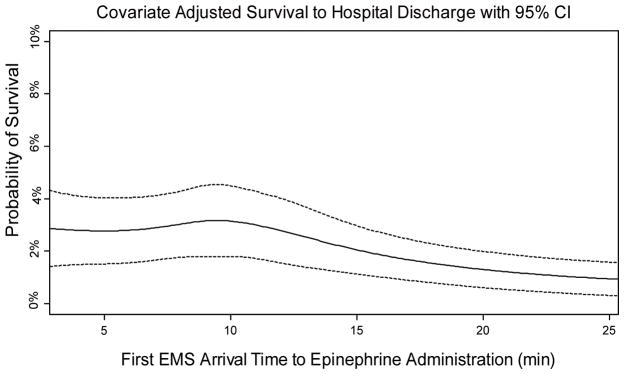
Results: From 55 568 EMS-treated OHCAs, 32 101 patients with initial nonshockable rhythms were included. There were 12 238 in the early group, 14 517 in the late group, and 5346 not treated with epinephrine. After adjusting for potential confounders, each minute from EMS arrival to epinephrine administration was associated with a 4% decrease in odds of survival for adults, odds ratio=0.96 (95% confidence interval, 0.95-0.98). A subgroup analysis (n=13 290) examining neurological outcomes showed a similar association (adjusted odds ratio, 0.94 per minute; 95% confidence interval, 0.89-0.98). When epinephrine was given late in comparison with early, odds of survival were 18% lower (odds ratio, 0.82; 95% confidence interval, 0.68-0.98). In a pediatric analysis (n=595), odds of survival were 9% lower (odds ratio, 0.91; 95% confidence interval, 0.81-1.01) for each minute delay in epinephrine.
Conclusions: Among OHCAs with nonshockable initial rhythms, the majority of patients were administered epinephrine >10 minutes after EMS arrival. Each minute delay in epinephrine administration was associated with decreased survival and unfavorable neurological outcomes. EMS agencies should consider strategies to reduce epinephrine administration times in patients with initial nonshockable rhythms.
Keywords: cardiopulmonary resuscitation; epinephrine; heart arrest; out-of-hospital cardiac arrest; resuscitation.
© 2018 American Heart Association, Inc.
Conflict of interest statement
None
Figures
References
-
- Cardiac Arrest Statistics [Internet] [cited 2017 Aug 7];Available from: http://cpr.heart.org/AHAECC/CPRAndECC/General/UCM_477263_Cardiac-Arrest-....
-
- Link MS, Berkow LC, Kudenchuk PJ, Halperin HR, Hess EP, Moitra VK, Neumar RW, O’Neil BJ, Paxton JH, Silvers SM, White RD, Yannopoulos D, Donnino MW. Part 7: Adult Advanced Cardiovascular Life Support. Circulation. 2015;132:S444–S464. - PubMed
-
- Olasveengen TM, Sunde K, Brunborg C, Thowsen J, Steen PA, Wik L. Intravenous drug administration during out-of-hospital cardiac arrest: a randomized trial. JAMA. 2009;302:2222–2229. - PubMed
-
- Jacobs IG, Finn JC, Jelinek GA, Oxer HF, Thompson PL. Effect of adrenaline on survival in out-of-hospital cardiac arrest: A randomised double-blind placebo-controlled trial. Resuscitation. 2011;82:1138–1143. - PubMed
-
- Hagihara A, Hasegawa M, Abe T, Nagata T, Wakata Y, Miyazaki S. Prehospital Epinephrine Use and Survival Among Patients With Out-of-Hospital Cardiac Arrest. JAMA. 2012;307:1161–1168. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077871/HL/NHLBI NIH HHS/United States
- K23 HL131440/HL/NHLBI NIH HHS/United States
- U01 HL077887/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- U01 HL077873/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- K12 HL108974/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
- CIHR/Canada
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
