

Increased risk of venous thromboembolism in hospitalized patients with cirrhosis due to non-alcoholic steatohepatitis
- PMID: 29511162
- PMCID: PMC5862151
- DOI: 10.1038/s41424-018-0002-y
Increased risk of venous thromboembolism in hospitalized patients with cirrhosis due to non-alcoholic steatohepatitis
Abstract
Objective: Patients with cirrhosis are at increased risk for venous thromboembolism (VTE) and portal vein thrombosis (PVT). Cirrhosis due to non-alcoholic steatohepatitis (NASH) appears to be particularly prothrombotic. We investigated hospitalized patients with NASH cirrhosis to determine if they are at increased risk for VTE.
Methods: Data on adult hospitalized patients with cirrhosis and VTE (deep vein thrombosis and/or pulmonary embolism) between November 1, 2010 and December 31, 2015 were obtained. Cases with VTE were matched by age, gender, and model for end stage liver disease (MELD) score to corresponding controls without VTE.
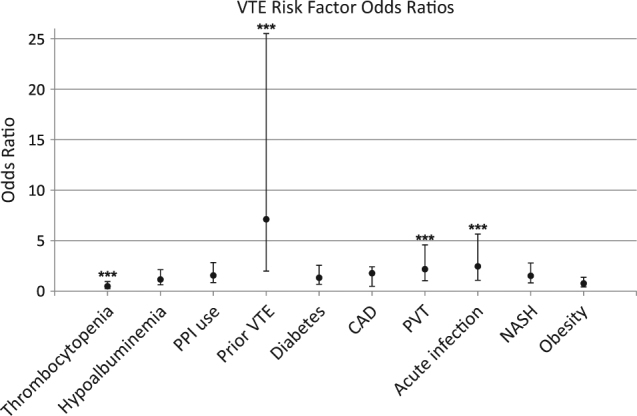
Results: Two hundred and ninety subjects (145 matched pairs) with mean age of 58.4 ± 11.8 years and MELD score of 16.0 ± 7.2 were included. Baseline characteristics were similar between cases and controls. Independent adjusted risk factors for VTE included NASH (OR: 2.46, 95% CI: 1.07-5.65, p = 0.034), prior VTE (OR: 7.12, 95% CI: 1.99-25.5, p = 0.003), and presence of PVT (OR: 2.18, 95% CI: 1.03-4.58, p = 0.041). Thrombocytopenia was associated with decreased risk (OR: 0.49, 95% CI: 0.26-0.95, p = 0.035).
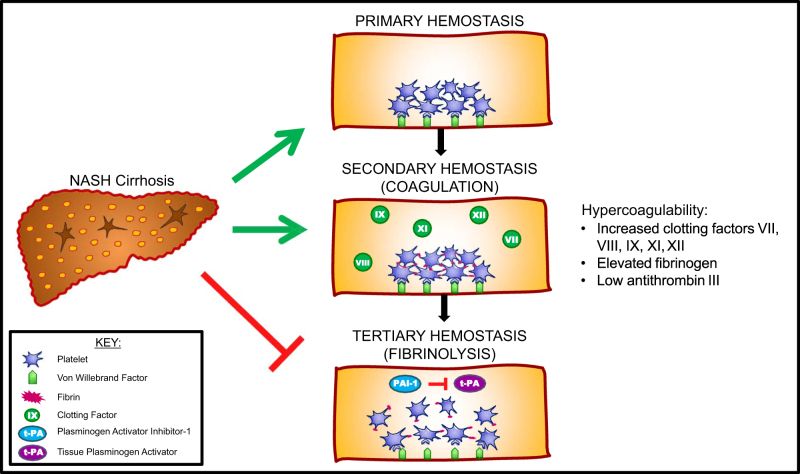
Conclusions: NASH is an independent risk factor for VTE among cirrhosis patients and provides further evidence that NASH is a hypercoagulable state. While all hospitalized patients with cirrhosis at risk for VTE should be considered for medical thromboprophylaxis, those with NASH cirrhosis are at particularly increased risk and therefore a high index of suspicion for VTE should be maintained even in the presence of thromboprophylaxis.
Conflict of interest statement
Figures
Similar articles
-
Impact of Cirrhosis Etiology on the Risk for Venous Thromboembolism.Dig Dis Sci. 2024 Jul;69(7):2691-2698. doi: 10.1007/s10620-024-08440-7. Epub 2024 May 3. Dig Dis Sci. 2024. PMID: 38700633
-
Case-control analysis of venous thromboembolism risk in non-alcoholic steatohepatitis diagnosed by transient elastography.World J Clin Cases. 2023 Dec 6;11(34):8126-8138. doi: 10.12998/wjcc.v11.i34.8126. World J Clin Cases. 2023. PMID: 38130793 Free PMC article.
-
Cirrhosis is Associated with an Increased 30-Day Mortality After Venous Thromboembolism.Clin Transl Gastroenterol. 2015 Jul 2;6(7):e97. doi: 10.1038/ctg.2015.27. Clin Transl Gastroenterol. 2015. PMID: 26133110 Free PMC article.
-
Risk factors for venous thromboembolism in children.Int Angiol. 2004 Sep;23(3):195-205. Int Angiol. 2004. PMID: 15765033 Review.
-
Prevention of venous thromboembolism in medical patients with thrombocytopenia or with platelet dysfunction: a review of the literature.Semin Thromb Hemost. 2011 Apr;37(3):267-74. doi: 10.1055/s-0031-1273090. Epub 2011 Mar 31. Semin Thromb Hemost. 2011. PMID: 21455860 Review.
Cited by
-
Anticoagulation in Patients with Liver Cirrhosis: Friend or Foe?Dig Dis Sci. 2023 Jun;68(6):2237-2246. doi: 10.1007/s10620-023-07858-9. Epub 2023 Mar 24. Dig Dis Sci. 2023. PMID: 36961672 Free PMC article. Review.
-
NASHFit: A randomized controlled trial of an exercise training program to reduce clotting risk in patients with NASH.Hepatology. 2022 Jul;76(1):172-185. doi: 10.1002/hep.32274. Epub 2022 Jan 22. Hepatology. 2022. PMID: 34890063 Free PMC article. Clinical Trial.
-
Plasminogen activator inhibitor is significantly elevated in liver transplant recipients with decompensated NASH cirrhosis.BMJ Open Gastroenterol. 2021 Jul;8(1):e000683. doi: 10.1136/bmjgast-2021-000683. BMJ Open Gastroenterol. 2021. PMID: 34341018 Free PMC article.
-
Impact of Cirrhosis Etiology on the Risk for Venous Thromboembolism.Dig Dis Sci. 2024 Jul;69(7):2691-2698. doi: 10.1007/s10620-024-08440-7. Epub 2024 May 3. Dig Dis Sci. 2024. PMID: 38700633
-
Global hemostatic profiling in patients with decompensated cirrhosis and bacterial infections.JHEP Rep. 2022 Apr 20;4(7):100493. doi: 10.1016/j.jhepr.2022.100493. eCollection 2022 Jul. JHEP Rep. 2022. PMID: 35647501 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
