

Variability of United States Online Rehabilitation Protocols for Proximal Hamstring Tendon Repair
- PMID: 29511700
- PMCID: PMC5826004
- DOI: 10.1177/2325967118755116
Variability of United States Online Rehabilitation Protocols for Proximal Hamstring Tendon Repair
Abstract
Background: The optimal postoperative rehabilitation protocol following repair of complete proximal hamstring tendon ruptures is the subject of ongoing investigation, with a need for more standardized regimens and evidence-based modalities.
Purpose: To assess the variability across proximal hamstring tendon repair rehabilitation protocols published online by United States (US) orthopaedic teaching programs.
Study design: Cross-sectional study.
Methods: Online proximal hamstring physical therapy protocols from US academic orthopaedic programs were reviewed. A web-based search using the search term complete proximal hamstring repair rehabilitation protocol provided an additional 14 protocols. A comprehensive scoring rubric was developed after review of all protocols and was used to assess each protocol for both the presence of various rehabilitation components and the point at which those components were introduced.
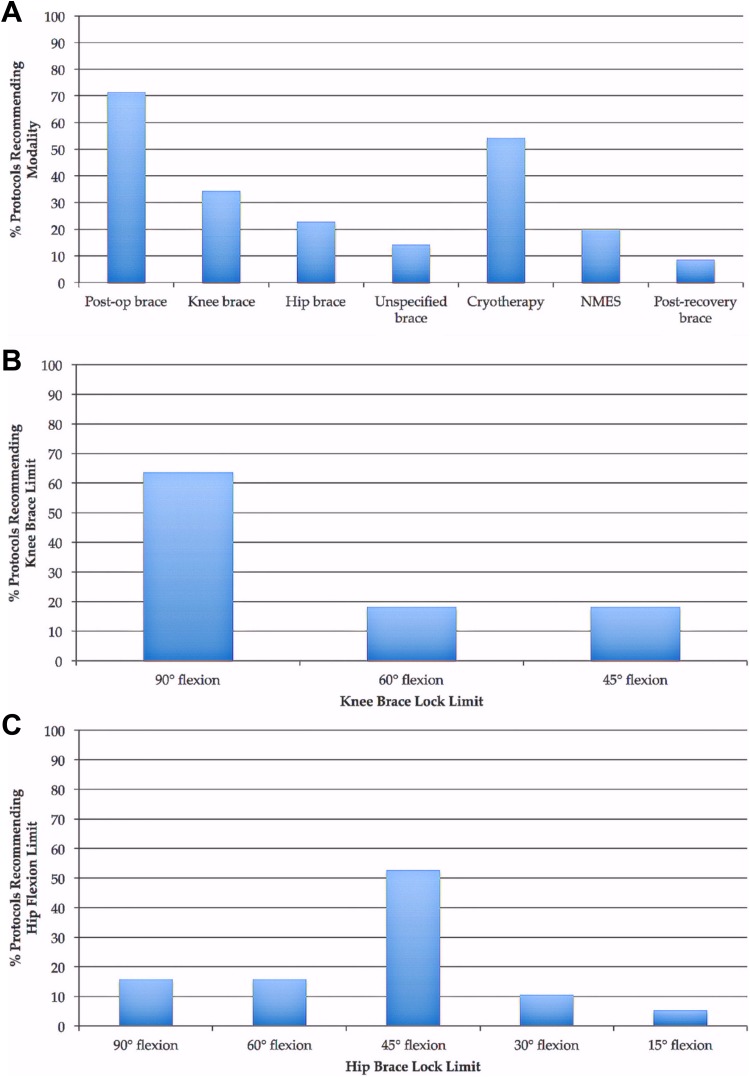
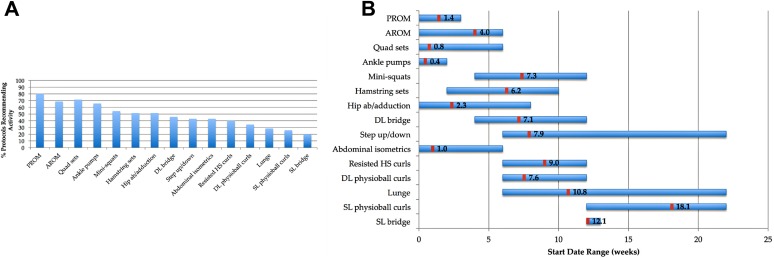
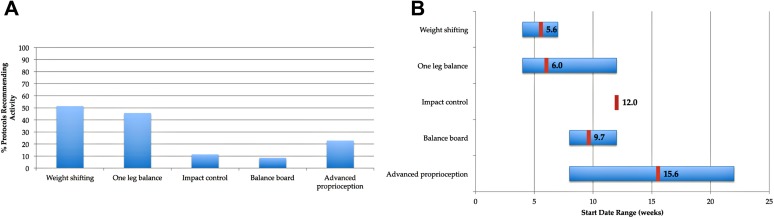
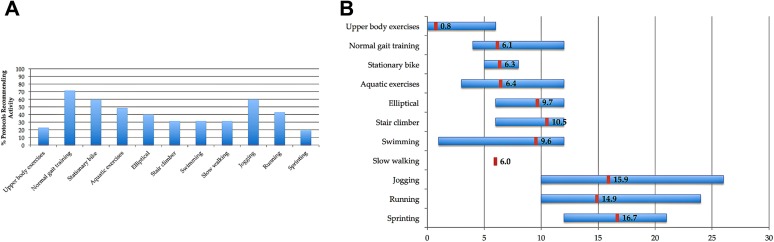
Results: Of 50 rehabilitation protocols identified, 35 satisfied inclusion criteria and were analyzed. Twenty-five protocols (71%) recommended immediate postoperative bracing: 12 (34%) prescribed knee bracing, 8 (23%) prescribed hip bracing, and 5 (14%) did not specify the type of brace recommended. Fourteen protocols (40%) advised immediate nonweightbearing with crutches, while 16 protocols (46%) permitted immediate toe-touch weightbearing. Advancement to full weightbearing was allowed at a mean of 7.1 weeks (range, 4-12 weeks). Most protocols (80%) recommended gentle knee and hip passive range of motion and active range of motion, starting at a mean 1.4 weeks (range, 0-3 weeks) and 4.0 weeks (range, 0-6 weeks), respectively. However, only 6 protocols (17%) provided specific time points to initiate full hip and knee range of motion: a mean 8.0 weeks (range, 4-12 weeks) and 7.8 weeks (range, 0-12 weeks), respectively. Considerable variability was noted in the inclusion and timing of strengthening, stretching, proprioception, and cardiovascular exercises. Fifteen protocols (43%) required completion of specific return-to-sport criteria before resuming training.
Conclusion: Marked variability is found in both the composition and timing of rehabilitation components across the various complete proximal hamstring repair rehabilitation protocols published online. This finding mirrors the variability of proposed rehabilitation protocols in the professional literature and represents an opportunity to improve patient care.
Keywords: hamstring; physical therapy; rehabilitation; tendon repair; tendon rupture.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: C.S.A. receives royalties from Arthrex; receives research support from Arthrex, Major League Baseball, and Stryker; has stock/stock options in At Peak; and receives publishing royalties from Lead Player.
Figures
Similar articles
-
Systematic Review of Bracing After Proximal Hamstring Repair.Orthop J Sports Med. 2024 Feb 23;12(2):23259671241230045. doi: 10.1177/23259671241230045. eCollection 2024 Feb. Orthop J Sports Med. 2024. PMID: 38405008 Free PMC article. Review.
-
Online Physical Therapy Protocol Quality, Variability, and Availability in Achilles Tendon Repair.Foot Ankle Spec. 2019 Feb;12(1):16-24. doi: 10.1177/1938640017751185. Epub 2018 Jan 8. Foot Ankle Spec. 2019. PMID: 29310456
-
Rehabilitation variability following medial patellofemoral ligament reconstruction.Phys Sportsmed. 2018 Nov;46(4):441-448. doi: 10.1080/00913847.2018.1487240. Epub 2018 Jul 2. Phys Sportsmed. 2018. PMID: 29888637
-
Quality and Variability of Online Physical Therapy Protocols for Isolated Meniscal Repairs.J Knee Surg. 2019 Jun;32(6):544-549. doi: 10.1055/s-0038-1655742. Epub 2018 May 31. J Knee Surg. 2019. PMID: 29852515
-
Quality and Variability of Online Available Physical Therapy Protocols From Academic Orthopaedic Surgery Programs for Medial Patellofemoral Ligament Reconstruction.Orthop J Sports Med. 2019 Jul 2;7(7):2325967119855991. doi: 10.1177/2325967119855991. eCollection 2019 Jul. Orthop J Sports Med. 2019. PMID: 31309124 Free PMC article. Review.
Cited by
-
Proximal Hamstring Ruptures: Treatment, Rehabilitation, and Return to Play.Curr Rev Musculoskelet Med. 2023 Mar;16(3):103-113. doi: 10.1007/s12178-023-09821-7. Epub 2023 Feb 9. Curr Rev Musculoskelet Med. 2023. PMID: 36757628 Free PMC article. Review.
-
Systematic Review of Bracing After Proximal Hamstring Repair.Orthop J Sports Med. 2024 Feb 23;12(2):23259671241230045. doi: 10.1177/23259671241230045. eCollection 2024 Feb. Orthop J Sports Med. 2024. PMID: 38405008 Free PMC article. Review.
-
Time required to achieve the minimal clinically important difference after open proximal hamstring repair.J Hip Preserv Surg. 2025 Jan 29;12(2):87-92. doi: 10.1093/jhps/hnae045. eCollection 2025 Jul. J Hip Preserv Surg. 2025. PMID: 40761576 Free PMC article.
-
Proximal Hamstring Injuries: Management of Tendinopathy and Avulsion Injuries.Curr Rev Musculoskelet Med. 2019 Jun;12(2):138-146. doi: 10.1007/s12178-019-09541-x. Curr Rev Musculoskelet Med. 2019. PMID: 30806898 Free PMC article. Review.
-
Rehabilitation Variability After Elbow Ulnar Collateral Ligament Reconstruction.Orthop J Sports Med. 2019 Mar 25;7(3):2325967119833363. doi: 10.1177/2325967119833363. eCollection 2019 Mar. Orthop J Sports Med. 2019. PMID: 30937318 Free PMC article.
References
-
- Askling CM, Koulouris G, Saartok T, Werner S, Best TM. Total proximal hamstring ruptures: clinical and MRI aspects including guidelines for postoperative rehabilitation. Knee Surg Sports Traumatol Arthrosc. 2013;21:515–533. - PubMed
-
- Bencardino JT, Mellado JM. Hamstring injuries of the hip. Magn Reson Imaging Clin N Am. 2005;13:677–690. - PubMed
-
- Birmingham P, Muller M, Wickiewicz T, Cavanaugh J, Rodeo S, Warren R. Functional outcome after repair of proximal hamstring avulsions. J Bone Joint Surg Am. 2011;93(19):1819–1826. - PubMed
-
- Blakeney WG, Zilko SR, Edmonston SJ, Schupp NE, Annear PT. A prospective evaluation of proximal hamstring tendon avulsions: improved functional outcomes following surgical repair. Knee Surg Sports Traumatol Arthrosc. 2017;25(6):1943–1950. - PubMed
-
- Blakeney WG, Zilko SR, Edmonston SJ, Schupp NE, Annear PT. Proximal hamstring tendon avulsion surgery: evaluation of the Perth Hamstring Assessment Tool. Knee Surg Sports Traumatol Arthrosc. 2017;25:1936–1942. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
