

Relationship Between Abdominal Symptoms and Fructose Ingestion in Children with Chronic Abdominal Pain
- PMID: 29511898
- PMCID: PMC5895692
- DOI: 10.1007/s10620-018-4997-4
Relationship Between Abdominal Symptoms and Fructose Ingestion in Children with Chronic Abdominal Pain
Erratum in
-
Correction to: Relationship Between Abdominal Symptoms and Fructose Ingestion in Children with Chronic Abdominal Pain.Dig Dis Sci. 2018 Jun;63(6):1670. doi: 10.1007/s10620-018-5046-z. Dig Dis Sci. 2018. PMID: 29611080 Free PMC article.
Abstract
Background: Limited valid data are available regarding the association of fructose-induced symptoms, fructose malabsorption, and clinical symptoms.
Aim: To develop a questionnaire for valid symptom assessment before and during a carbohydrate breath test and to correlate symptoms with fructose breath test results in children/adolescents with functional abdominal pain.
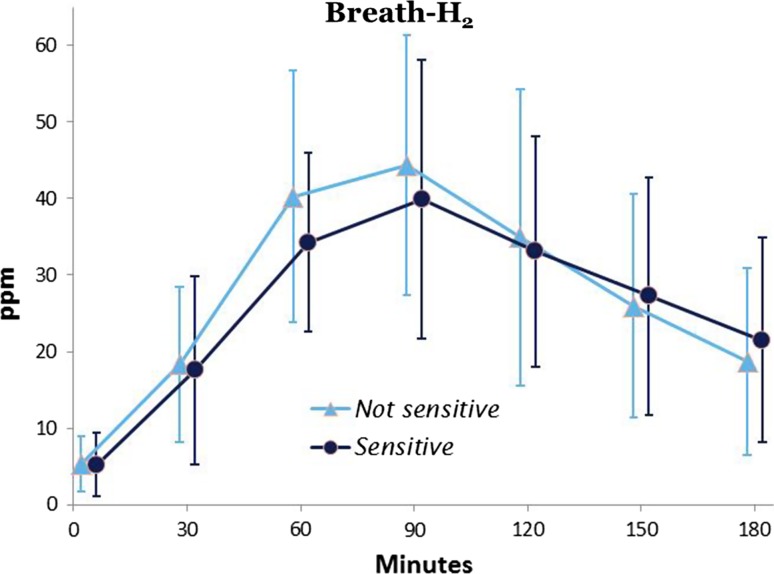
Methods: A Likert-type questionnaire assessing symptoms considered relevant for hydrogen breath test in children was developed and underwent initial validation. Fructose malabsorption was determined by increased breath hydrogen in 82 pediatric patients with functional abdominal pain disorders; fructose-induced symptoms were quantified by symptom score ≥2 and relevant symptom increase over baseline. The results were correlated with clinical symptoms. The time course of symptoms during the breath test was assessed.
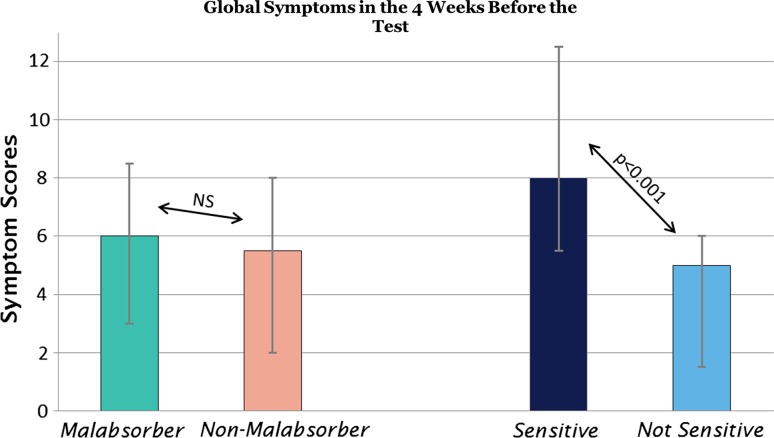
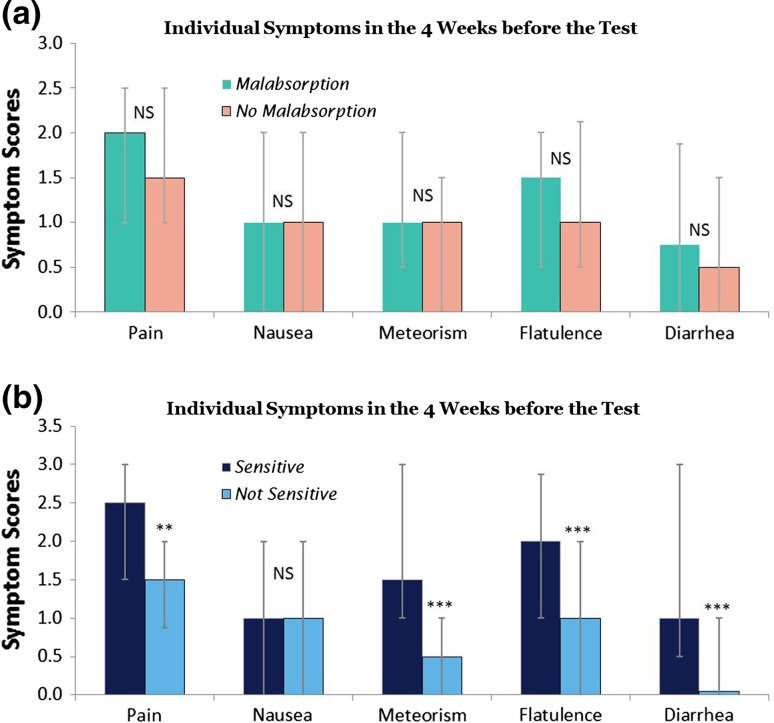
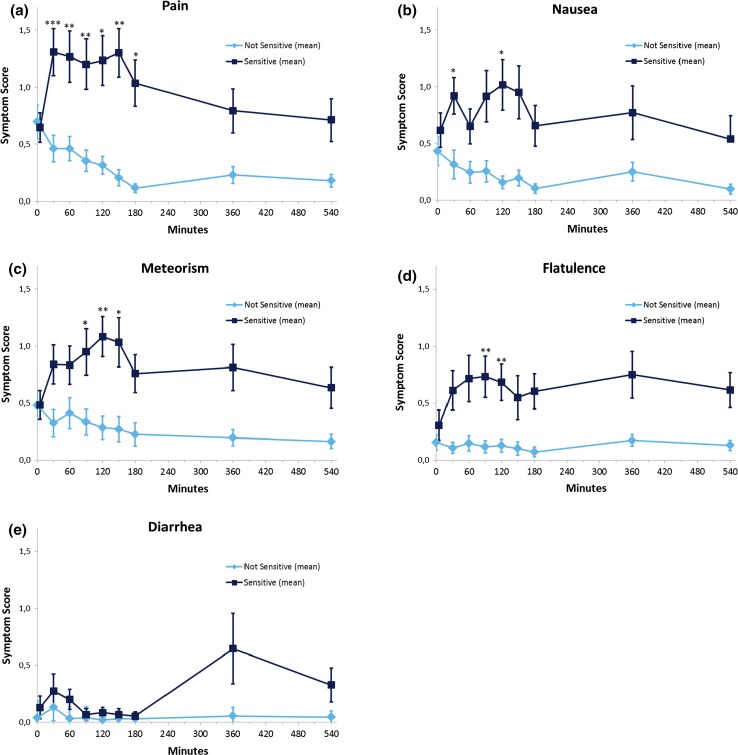
Results: The questionnaire exhibited good psychometric properties in a standardized assessment of the severity of carbohydrate-related symptoms. A total of 40 % (n = 33) had malabsorption; symptoms were induced in 38 % (n = 31), but only 46 % (n = 15) with malabsorption were symptomatic. There was no significant correlation between fructose malabsorption and fructose-induced symptoms. Clinical symptoms correlated with symptoms evoked during the breath test (p < 0.001, r2 = 0.21) but not with malabsorption (NS). Malabsorbers did not differ from non-malabsorbers in terms of symptoms during breath test. Symptomatic patients had significantly higher pain and flatulence scores over the 9-h observation period (p < 0.01) than did nonsymptomatic patients; the meteorism score was higher after 90 min.
Conclusions: Fructose-induced symptoms but not fructose malabsorption are related to increased abdominal symptoms and have distinct timing patterns.
Keywords: Adolescents; Children; Fructose malabsorption; Functional abdominal pain; Hypersensitivity.
Conflict of interest statement
Conflict of interest
No conflicts of interest exist.
Provision of questionnaires
For studies without financial support from industrial sponsors, we provide the questionnaires free of charge.
Figures
References
-
- DiLorenzo C, Hyams J, Saps M, et al. et al. Childhood functional gastrointestinal disorders, child/adolescent. In: Drossman D, Chang L, Chey W, et al.et al., editors. Rome IV, Functional Gastrointestinal Disorders, Disorders of Gut-Brain Interaction. Raleigh, NC: The Rome Foundation; 2016. pp. 1297–1371.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
