

Lymphopenia is associated with late onset Pneumocystis jirovecii pneumonia in solid organ transplantation
- PMID: 29512868
- PMCID: PMC11812524
- DOI: 10.1111/tid.12876
Lymphopenia is associated with late onset Pneumocystis jirovecii pneumonia in solid organ transplantation
Abstract
Background: Pneumocystis jirovecii pneumonia (PJP) affected 5%-15% of solid organ transplant (SOT) recipients prior to universal prophylaxis, classically with trimethoprim-sulfamethoxazole (TMP-SMX). Guidelines generally recommend 6-12 months of prophylaxis post-SOT, yet optimal duration and robust PJP risk stratification have not been established.
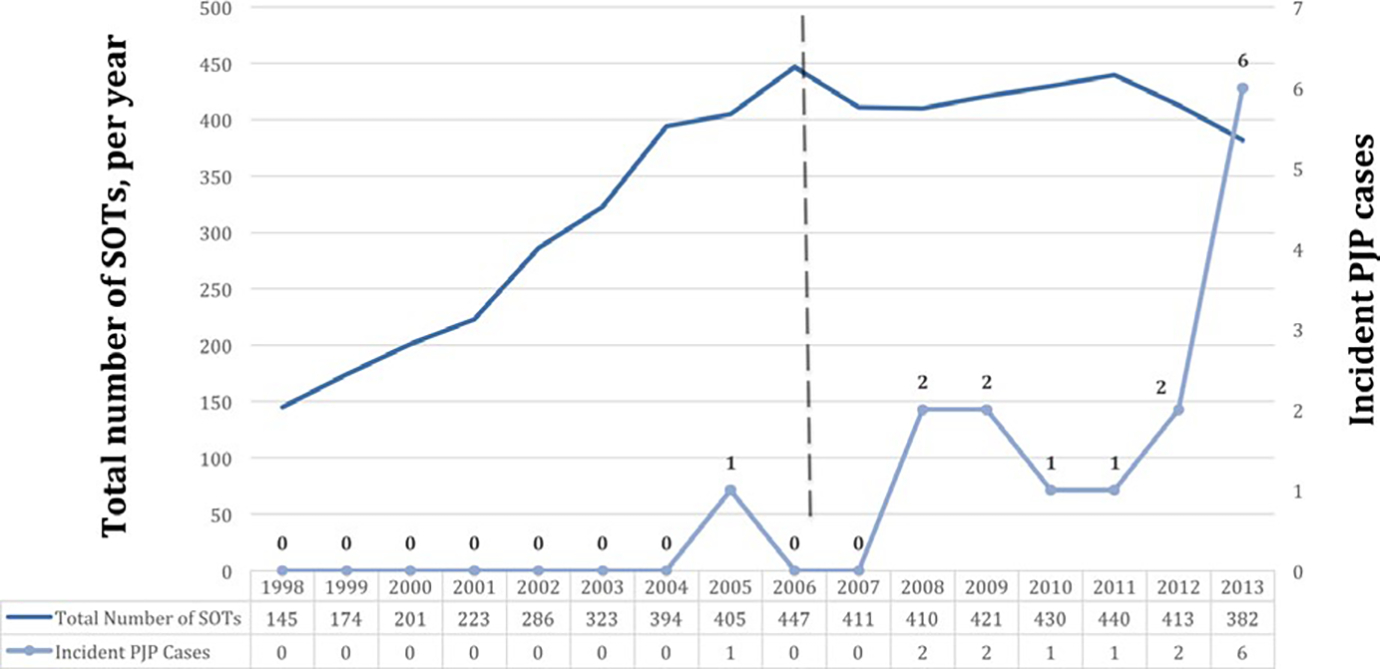
Methods: A retrospective, single-center, case-control study of PJP among SOT recipients from January 1998 to December 2013 was conducted. Cases had positive PJ direct fluorescent antibody assay of respiratory specimens. Controls were matched 4:1 by nearest date of SOT. Univariate testing and multivariate logistic regressions were performed.
Results: Fifteen cases were identified among 5505 SOT recipients (0.27% rate) and analyzed vs 60 controls. PJP occurred on average 6.1 years (range 0.9-13.8) post-SOT; no case was receiving PJP prophylaxis at diagnosis. Most were treated with reduced immunosuppression and TMP-SMX plus steroids (80%). Six patients (40%) required critical care; 3 (20%) died. There were no significant demographic differences, though cases tended to be older at SOT (54 vs 48 years, P = .1). In univariate analysis, prior viral infection was more common among cases (67% vs 37%, P = .08). Lower absolute lymphocyte count (ALC) at diagnosis date was strongly associated with PJP (400 vs 1230 × 106 cells/μL, P < .001); odds of infection were high with ALC ≤ 500 × 106 cells (OR 18.7, P < .01).
Conclusion: Pneumocystis jirovecii pneumonia is a rare, late complication of SOT with significant morbidity and mortality. Severe lymphopenia may be useful in identifying SOT recipients who warrant continued or reinstated PJP prophylaxis.
Keywords: Pneumocystis; organ transplantation; pneumonia; prophylaxis.
© 2018 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Figures
Similar articles
-
Pneumocystis jirovecii pneumonia in solid organ transplant recipients: a descriptive analysis for the Swiss Transplant Cohort.Transpl Infect Dis. 2018 Dec;20(6):e12984. doi: 10.1111/tid.12984. Epub 2018 Sep 19. Transpl Infect Dis. 2018. PMID: 30155950
-
A Comprehensive Evaluation of Risk Factors for Pneumocystis jirovecii Pneumonia in Adult Solid Organ Transplant Recipients: A Systematic Review and Meta-analysis.Transplantation. 2021 Oct 1;105(10):2291-2306. doi: 10.1097/TP.0000000000003576. Transplantation. 2021. PMID: 33323766
-
Risk factors and outcomes of Pneumocystis pneumonia in solid organ transplant recipients: Impact of posttransplant lymphoproliferative disorder.Clin Transplant. 2023 Sep;37(9):e15021. doi: 10.1111/ctr.15021. Epub 2023 May 17. Clin Transplant. 2023. PMID: 37195184 Free PMC article.
-
Alternative Pneumocystis Pneumonia Prophylaxis in Solid Organ Transplants.Transpl Infect Dis. 2025 Jan-Feb;27(1):e14410. doi: 10.1111/tid.14410. Epub 2024 Nov 27. Transpl Infect Dis. 2025. PMID: 39603840 Free PMC article.
-
Prophylaxis and treatment of Pneumocystis Jirovecii pneumonia after solid organ transplantation.Pharmacol Res. 2018 Aug;134:61-67. doi: 10.1016/j.phrs.2018.06.010. Epub 2018 Jun 8. Pharmacol Res. 2018. PMID: 29890253 Review.
Cited by
-
Risk factors for Pneumocystis pneumonia with acute respiratory failure among kidney transplant recipients.BMC Nephrol. 2023 Feb 9;24(1):31. doi: 10.1186/s12882-023-03071-y. BMC Nephrol. 2023. PMID: 36759777 Free PMC article.
-
Diagnostic and therapeutic approach to infectious diseases in solid organ transplant recipients.Intensive Care Med. 2019 May;45(5):573-591. doi: 10.1007/s00134-019-05597-y. Epub 2019 Mar 25. Intensive Care Med. 2019. PMID: 30911807 Free PMC article. Review.
-
Pneumocystis jirovecii pneumonia in non-HIV patients: need for a more extended prophylaxis.Front Med (Lausanne). 2024 Jun 26;11:1414092. doi: 10.3389/fmed.2024.1414092. eCollection 2024. Front Med (Lausanne). 2024. PMID: 38988362 Free PMC article.
-
Pneumocystis jirevocii and SARS-CoV-2 Co-Infection: A Common Feature in Transplant Recipients?Vaccines (Basel). 2020 Sep 18;8(3):544. doi: 10.3390/vaccines8030544. Vaccines (Basel). 2020. PMID: 32962148 Free PMC article.
-
Neutropenia and Infection Prophylaxis in Childhood Cancer.Curr Oncol Rep. 2022 Jun;24(6):671-686. doi: 10.1007/s11912-022-01192-5. Epub 2022 Mar 1. Curr Oncol Rep. 2022. PMID: 35230594 Free PMC article. Review.
References
-
- Gordon SM, LaRosa SP, Kalmadi S, et al. Should prophylaxis for Pneumocystis carinii pneumonia in solid organ transplant recipients ever be discontinued? Clin Infect Dis. 1999;28:240–246. - PubMed
-
- Hibberd PL, Tolkoff-Rubin NE, Doran M, et al. Trimethoprim-sulfamethoxazole compared with ciprofloxacin for the prevention of urinary tract infection in renal transplant recipients. A double-blind, randomized controlled trial. Online J Curr Clin Trials. 1992;Doc No 15:[4083 words; 4046 paragraphs]. - PubMed
-
- Olsen SL, Renlund DG, O’Connell JB, et al. Prevention of Pneumocystis carinii pneumonia in cardiac transplant recipients by trimethoprim sulfamethoxazole. Transplantation. 1993;56:359–362. - PubMed
-
- Kostakis ID, Sotiropoulos GC, Kouraklis G. Pneumocystis jirovecii pneumonia in liver transplant recipients: a systematic review. Transplant. Proc. 2014;46:3206–3208. - PubMed
-
- Pappas PG, Alexander BD, Andes DR, et al. Invasive fungal infections among organ transplant recipients: results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin Infect Dis. 2010;50:1101–1111. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
