

A care bundle including antenatal corticosteroids reduces preterm infant mortality in Tanzania a low resource country
- PMID: 29513706
- PMCID: PMC5841752
- DOI: 10.1371/journal.pone.0193146
A care bundle including antenatal corticosteroids reduces preterm infant mortality in Tanzania a low resource country
Abstract
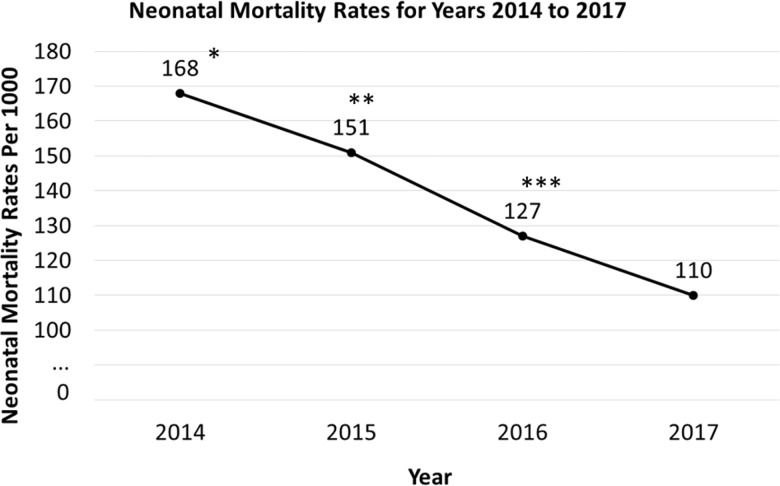
Background: Preterm neonatal mortality (NM) has remained high and unchanged for many years in Tanzania, a resource-limited country. Major causes of mortality include birth asphyxia, respiratory insufficiency and infections. Antenatal corticosteroids (ACS) have been shown to significantly reduce mortality in developed countries. There is inconsistent use of ACS in Tanzania.
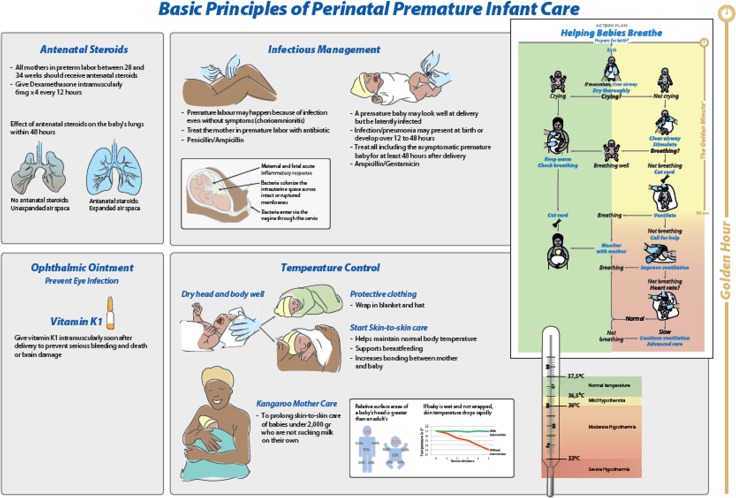
Objective: To determine whether implementation of a care bundle that includes ACS, maternal antibiotics (MA), neonatal antibiotics (NA) and avoidance of moderate hypothermia (temperature < 36°C) targeting infants of estimated gestational age (EGA) 28 to 34 6/7 weeks would reduce NM (< 7 days) by 35%.
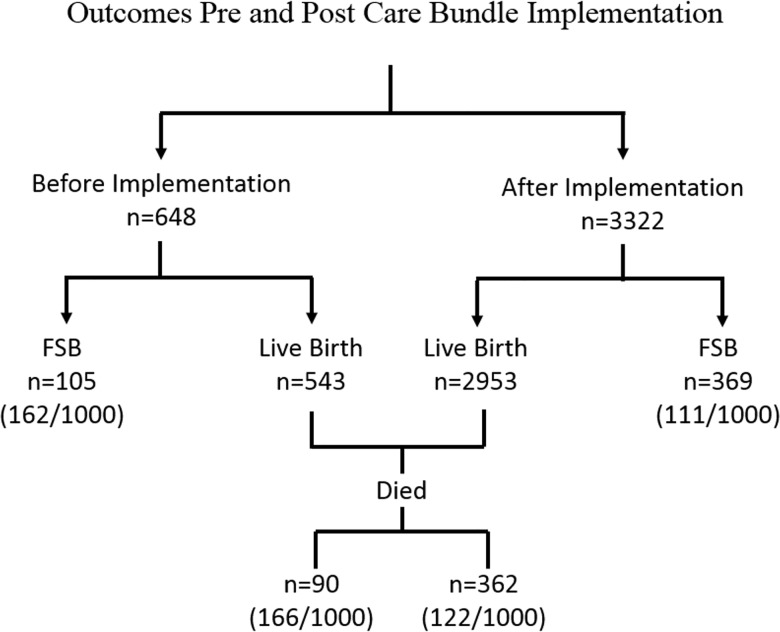
Methods: A Pre (September 2014 to May 2015) and Post (June 2015 to June 2017) Implementation strategy was used and introduced at three University-affiliated and one District Hospital. Dexamethasone, as the ACS, was added to the national formulary in May 2015, facilitating its free use down to the district level.
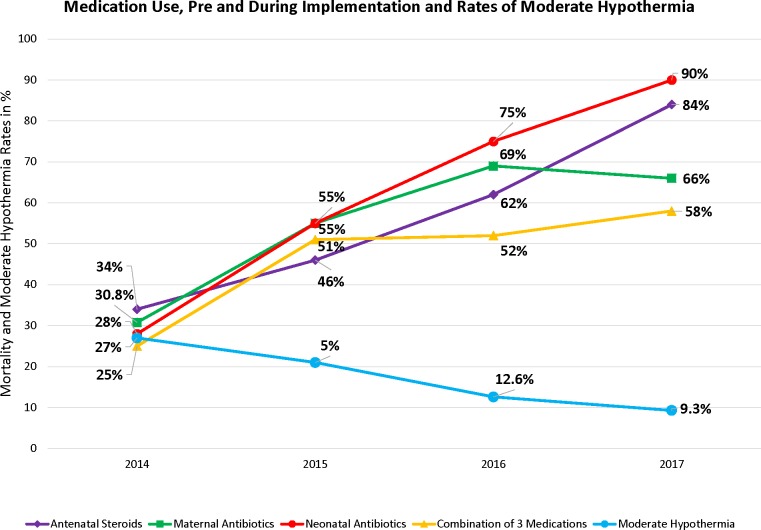
Findings: NM was reduced 26% from 166 to 122/1000 livebirths (P = 0.005) and fresh stillbirths (FSB) 33% from 162/1000 to 111/1000 (p = 0.0002) Pre versus Post Implementation. Medications including combinations increased significantly at all sites (p<0.0001). By logistic regression, combinations of ACS, maternal and NA (odds ratio (OR) 0.33), ACS and NA (OR 0.30) versus no treatment were significantly associated with reduced NM. NM significantly decreased per 250g birthweight increase (OR 0.59), and per one week increase in EGA (OR 0.87). Moderate hypothermia declined pre versus post implementation (p<0.0001) and was two-fold more common in infants who died versus survivors.
Interpretation: A low-cost care bundle, ~$6 per patient, was associated with a significant reduction in NM and FSB rates. The former presumably by reducing respiratory morbidity with ACS and minimizing infections with antibiotics. If these findings can be replicated in other resource-limited settings, the potential for further reduction of <5 year mortality rates becomes enormous.
Conflict of interest statement
Figures
References
-
- UNICEF/WHO/The World Bank/UN Pop Div. Levels and Trends in Child Mortality. Report 2014. Available from: http://www.who.int/maternal_child_adolescent/documents/levels_trends_chi...
-
- Liu L, Oza S, Hogan D, Perin J, Rudan I, Lawn JE, et al. Global, regional, and national causes of child mortality in 2000–13, with projections to inform post-2015 priorities: an updated systematic analysis. Lancet. 2015;385(9966): 430–40. doi: 10.1016/S0140-6736(14)61698-6 Epub 2014 Sep 30. - DOI - PubMed
-
- You D, Hug L, Chen Y, Wardlaw T, Newby H. Levels & Trends in Child Mortality. 2014. Available from: https://www.unicef.org/media/files/Levels_and_Trends_in_Child_Mortality_.... Accessed May 1, 2017.
-
- Msemo G, Massawe A, Mmbando D, Rusibamayila N, Manji K, Kidando H, et al. Newborn Mortality and Fresh Stillbirth Rates in Tanzania after Helping Babies Breathe Training. Pediatrics. 2013; 131(2): e353–60. doi: 10.1542/peds.2012-1795 - DOI - PubMed
-
- Antenatal corticosteroid therapy for fetal maturation. Committee Opinion No. 677. Obstet Gynecol. 2016; 128: e187–94. doi: 10.1097/AOG.0000000000001715 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
