

Impact of universal medical insurance system on the accessibility of medical service supply and affordability of patients in China
- PMID: 29513712
- PMCID: PMC5841764
- DOI: 10.1371/journal.pone.0193273
Impact of universal medical insurance system on the accessibility of medical service supply and affordability of patients in China
Abstract
Background: China's universal medical insurance system (UMIS) is designed to promote social fairness through improving access to medical services and reducing out-of-pocket (OOP) costs for all Chinese. However, it is still not known whether UMIS has a significant impact on the accessibility of medical service supply and the affordability, as well as the seeking-care choice, of patients in China.
Methods: Segmented time-series regression analysis, as a powerful statistical method of interrupted time series design, was used to estimate the changes in the quantity and quality of medical service supply before and after the implementation of UMIS. The rates of catastrophic payments and seeking-care choices for UMIS beneficiaries were selected to measure the affordability and medical service flow of patients after the implementation of UMIS.
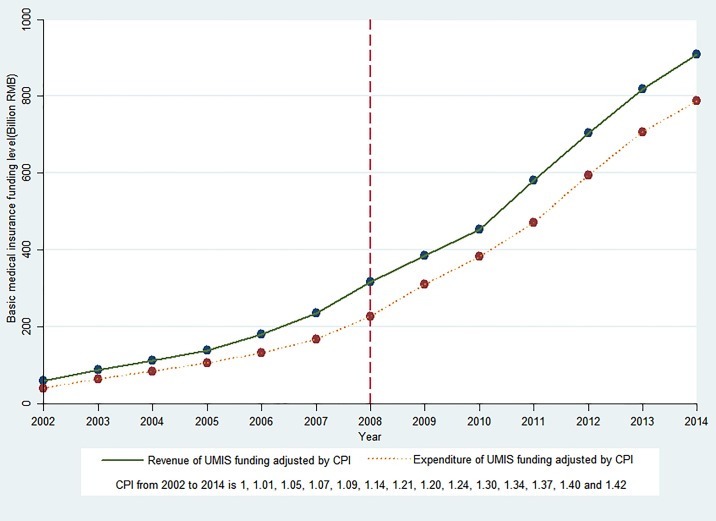
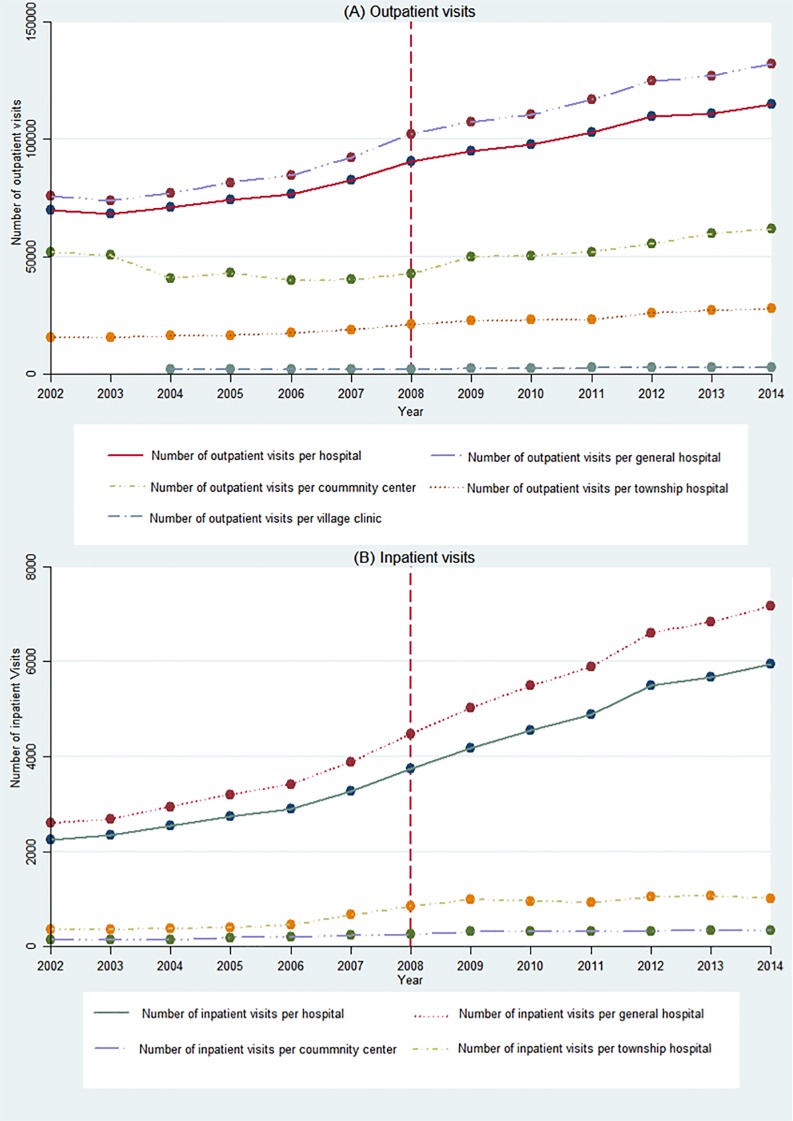
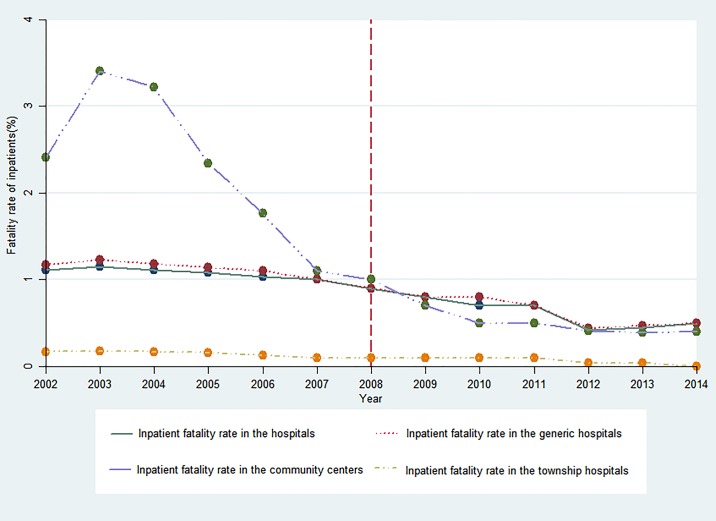
Results: China's UMIS was established in 2008. After that, the trending increase of the expenditure of the UMIS was higher than that of increase in revenue compared to previous years. Up to 2014, the UMIS had covered 97.5% of the entire population in China. After introduction of the UMIS, there were significant increases in licensed physicians, nurses, and hospital beds per 1000 individuals. In addition, hospital outpatient visits and inpatient visits per year increased compared to the pre-UMIS period. The average fatality rate of inpatients in the overall hospital and general hospital and the average fatality rate due to acute myocardial infarction (AMI) in general hospitals was significantly decreased. In contrast, no significant and prospective changes were observed in rural physicians per 1000 individuals, inpatient visits and inpatient fatality rate in the community centers and township hospitals compared to the pre-UMIS period. After 2008, the rates of catastrophic payments for UMIS inpatients at different income levels were declining at three levels of hospitals. Whichever income level, the rate of catastrophic payments for inpatients of Urban Employee's Basic Medical Insurance was the lowest. For the low-income patients, a single hospitalization at a tertiary hospital can lead to catastrophic payments. It is needless to say what the economic burden could be if patients required multiple hospitalizations within a year. UMIS beneficiaries showed the intention of growth to seek hospitalization services in tertiary hospitals.
Conclusions: Introduction of the UMIS contributed to an increase in available medical services and the use thereof, and a decrease in fatality rate. The affordability of UMIS beneficiaries for medical expenses was successfully ameliorated. The differences in patients' affordability are mainly manifested in different medical insurance schemes and different seeking-care choices. The ability of the poor patients covered by UMIS to resist catastrophic medical payments is still relatively weak. Therefore, the current UMIS should reform the insurance payment model to promote the integration of medical services and the formation of a tiered treatment system. UMIS also should establish supplementary medical insurance packages for the poor.
Conflict of interest statement
Figures
References
-
- Filipski MJ, Zhang Y, Chen KZ. Making health insurance pro-poor: evidence from a household panel in rural China. BMC HEALTH SERV RES, 2015;15(1):1–13. doi: 10.1186/s12913-015-0871-7 - DOI - PMC - PubMed
-
- Liu Y. Reforming China’s urban health insurance system. HEALTH POLICY, 2002;60(2):133–50. doi: 10.1016/S0168-8510(01)00207-X - DOI - PubMed
-
- Fang P, Dong S, Xiao J. The Institutional Change and Approach Choice of Governmental Health Input in China. Wuhan University Journal (Philosophy & Social Sciences), 2009;62(2):201–12. (Chinese)
-
- Tian X. Reflections on the Establishment of China’s Medical Insurance System. Chinese Health Economics, 1990;09(05):11–3. (Chinese)
-
- Yu H. Universal health insurance coverage for 1.3 billion people: What accounts for China’s success? HEALTH POLICY, 2015;119(9):1145–52. doi: 10.1016/j.healthpol.2015.07.008 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
