

MR Imaging of Rectal Cancer: Radiomics Analysis to Assess Treatment Response after Neoadjuvant Therapy
- PMID: 29514017
- PMCID: PMC5978457
- DOI: 10.1148/radiol.2018172300
MR Imaging of Rectal Cancer: Radiomics Analysis to Assess Treatment Response after Neoadjuvant Therapy
Abstract
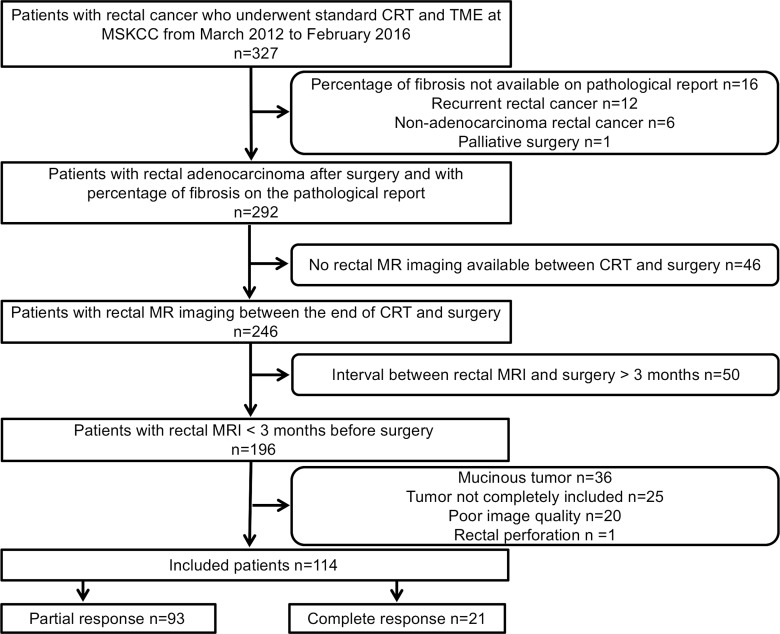
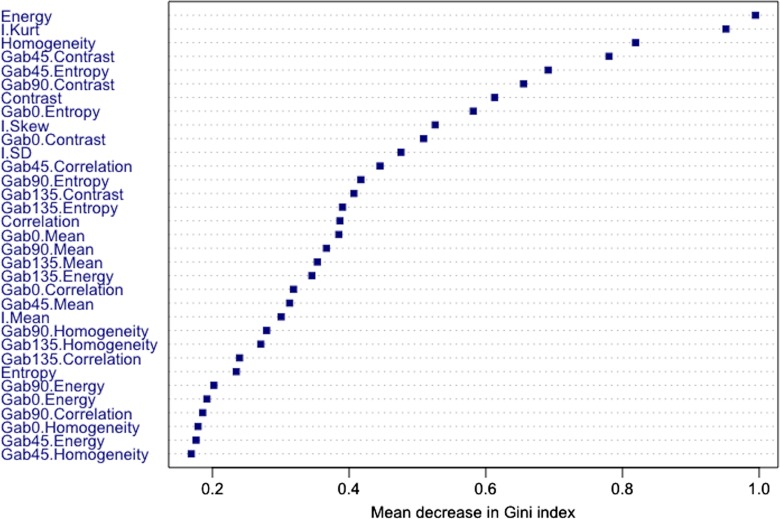
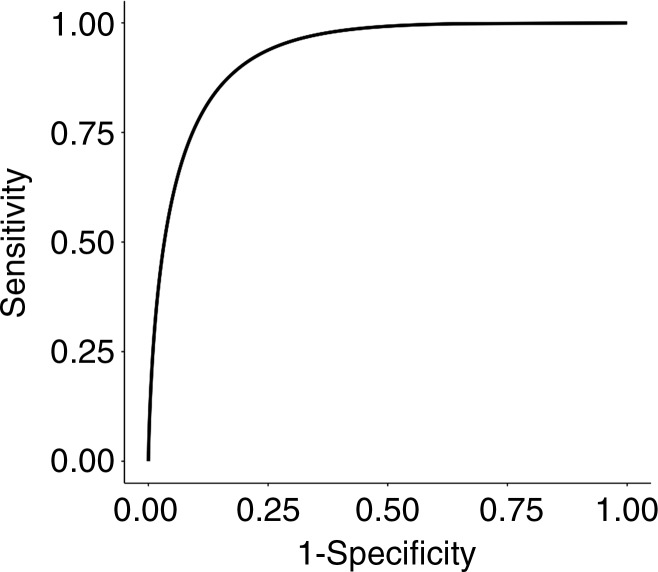
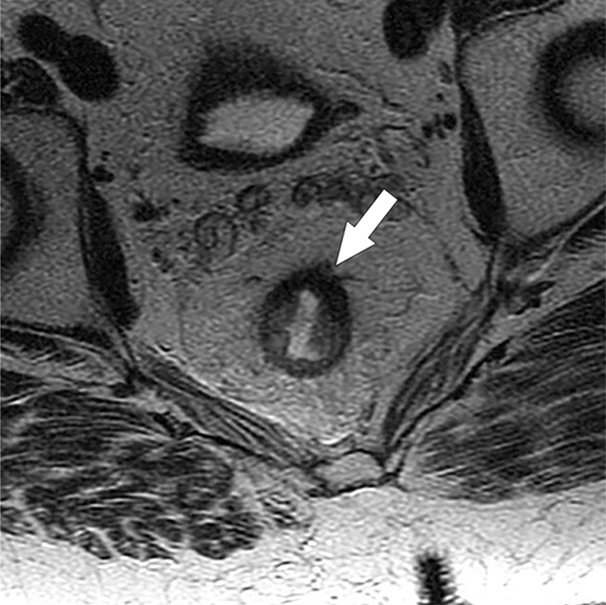
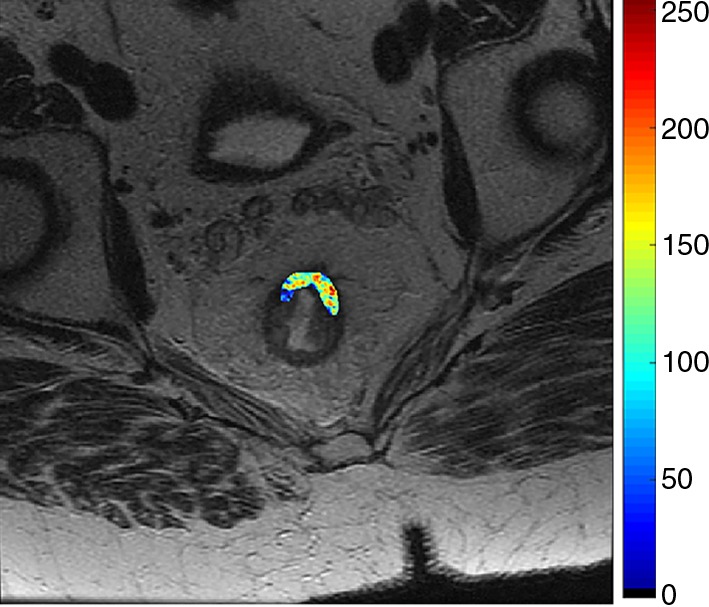
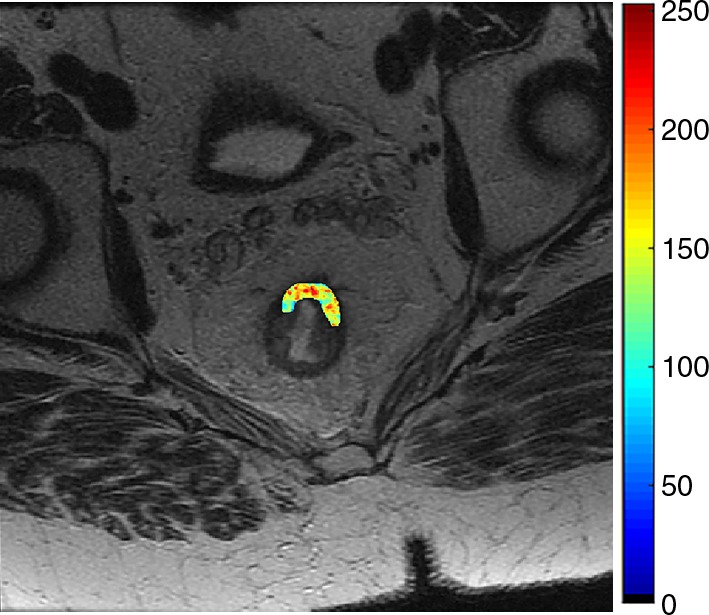
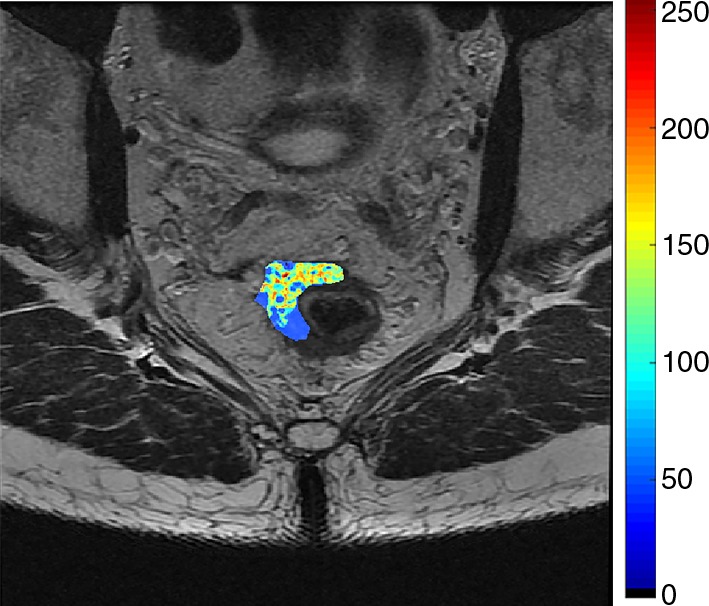
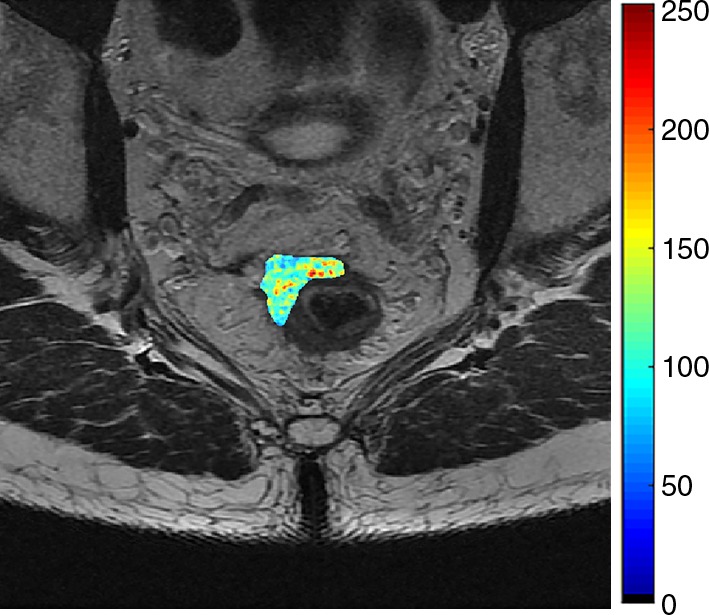
Purpose To investigate the value of T2-weighted-based radiomics compared with qualitative assessment at T2-weighted imaging and diffusion-weighted (DW) imaging for diagnosis of clinical complete response in patients with rectal cancer after neoadjuvant chemotherapy-radiation therapy (CRT). Materials and Methods This retrospective study included 114 patients with rectal cancer who underwent magnetic resonance (MR) imaging after CRT between March 2012 and February 2016. Median age among women (47 of 114, 41%) was 55.9 years (interquartile range, 45.4-66.7 years) and median age among men (67 of 114, 59%) was 55 years (interquartile range, 48-67 years). Surgical histopathologic analysis was the reference standard for pathologic complete response (pCR). For qualitative assessment, two radiologists reached a consensus. For radiomics, one radiologist segmented the volume of interest on high-spatial-resolution T2-weighted images. A random forest classifier was trained to separate the patients by their outcomes after balancing the number of patients in each response category by using the synthetic minority oversampling technique. Statistical analysis was performed by using the Wilcoxon rank-sum test, McNemar test, and Benjamini-Hochberg method. Results Twenty-one of 114 patients (18%) achieved pCR. The radiomic classifier demonstrated an area under the curve of 0.93 (95% confidence interval [CI]: 0.87, 0.96), sensitivity of 100% (95% CI: 0.84, 1), specificity of 91% (95% CI: 0.84, 0.96), positive predictive value of 72% (95% CI: 0.53, 0.87), and negative predictive value of 100% (95% CI: 0.96, 1). The diagnostic performance of radiomics was significantly higher than was qualitative assessment at T2-weighted imaging or DW imaging alone (P < .02). The specificity and positive predictive values were significantly higher in radiomics than were at combined T2-weighted and DW imaging (P < .0001). Conclusion T2-weighted-based radiomics showed better classification performance compared with qualitative assessment at T2-weighted and DW imaging for diagnosing pCR in patients with locally advanced rectal cancer after CRT. © RSNA, 2018 Online supplemental material is available for this article.
Figures



References
-
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet 1986;1(8496):1479–1482. - PubMed
-
- Krook JE, Moertel CG, Gunderson LL, et al. . Effective surgical adjuvant therapy for high-risk rectal carcinoma. N Engl J Med 1991;324(11):709–715. - PubMed
-
- Gastrointestinal Tumor Study Group . Prolongation of the disease-free interval in surgically treated rectal carcinoma. N Engl J Med 1985;312(23):1465–1472. - PubMed
-
- Adjuvant therapy for patients with colon and rectum cancer. Consens Statement 1990;8(4):1–25. - PubMed
-
- Sauer R, Becker H, Hohenberger W, et al. . Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med 2004;351(17):1731–1740. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
