

Predictive value of spot versus 24-hour measures of proteinuria for death, end-stage kidney disease or chronic kidney disease progression
- PMID: 29514605
- PMCID: PMC5842596
- DOI: 10.1186/s12882-018-0853-1
Predictive value of spot versus 24-hour measures of proteinuria for death, end-stage kidney disease or chronic kidney disease progression
Abstract
Background: Proteinuria is well recognised as a marker of chronic kidney disease (CKD), as a risk factor for progression of CKD among those with known CKD, and as a risk factor for cardiovascular events and death among both the general and CKD populations. Which measure of proteinuria is most predictive of renal events remains uncertain.
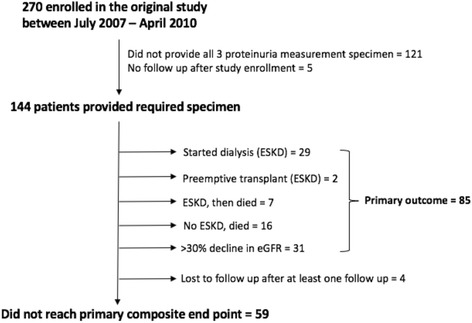
Methods: We conducted a prospective study with 144 proteinuric CKD and kidney transplant recipients attending an outpatient clinic of a tertiary care hospital in Australia. We concurrently collected morning spot urine protein-to-creatinine ratio (UPCR), albumin-to-creatinine ratio (UACR) and 24-h urinary protein excretion (24-UPE) from each participant at baseline. The primary outcome was a composite of death, ESKD or > 30% decline in eGFR over 5-years. Secondary outcomes were each component of the composite outcome. For each proteinuria measure, we performed a Cox Proportional Hazards model and calculated the Harrell's C-statistic and Akaike's Information Criterion (AIC).
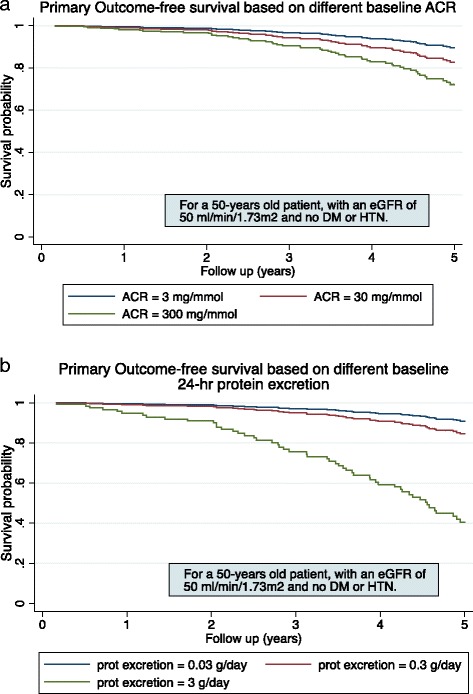
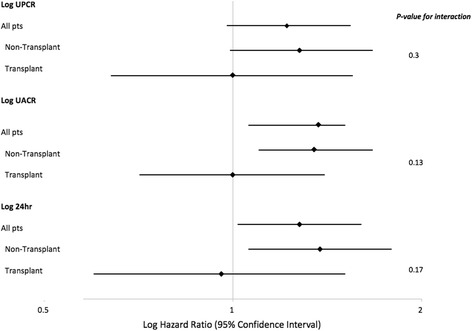
Results: After a mean follow-up of 5 years (range 4.4-6), 85 (59%) patients met the primary composite outcome including 23 deaths (16%). The multivariable analysis showed strong evidence of an association between each log-transformed proteinuria measurement and the primary composite outcome. [Log-UPCR 1.31 (95% CI 1.18-1.63), log-UACR 1.27 (1.11-1.45) and log-24-UPE 1.43 (1.20-1.71)]. The C-Statistic were similar for all three measures of proteinuria [UPCR: 0.74 (95% CI: 0.69-0.80), UACR: 0.75 (0.69-0.81), 24-UPE: 0.75 (0.69-0.81)] as were the models' AIC (671, 668 and 665 respectively). For secondary outcomes, no proteinuria measure was significantly associated with death alone ([log-UPCR = 1.18 (0.96-1.84), log-UACR = 1.19 (1.00-1.55), log-24-UPE = 1.19 (0.83-1.71)], whilst UACR and 24-UPE demonstrated marginally better association with ESKD and > 30% decline in eGFR respectively. [For ESKD, adj log-UACR HR = 1.33 (1.07-1.66). For > 30% decline in eGFR, log-24-UPE adj HR = 1.54 (1.13-2.09)].
Conclusion: In patients with stable, non-nephrotic CKD, all three measures of proteinuria were similarly predictive of hard clinical endpoints, defined as a composite of death, ESKD and > 30% decline in eGFR. However, which measure best predicted the outcomes individually is less certain.
Keywords: Albumin-to-creatinine ratio; Albuminuria; Chronic kidney disease; Protein-to-creatinine ratio; Proteinuria; Renal outcomes.
Conflict of interest statement
Ethics approval and consent to participate
All patients gave written consent for their participation in the study. The Sydney Local Area Health district ethics committee approved the study (protocol no. X16–0269).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Predicting kidney transplantation outcomes using proteinuria ascertained from spot urine samples versus timed urine collections.Am J Kidney Dis. 2014 Dec;64(6):962-8. doi: 10.1053/j.ajkd.2014.07.027. Epub 2014 Oct 8. Am J Kidney Dis. 2014. PMID: 25304983
-
Urinary neutrophil gelatinase-associated lipocalin may aid prediction of renal decline in patients with non-proteinuric Stages 3 and 4 chronic kidney disease (CKD).Nephrol Dial Transplant. 2013 Jun;28(6):1569-79. doi: 10.1093/ndt/gfs586. Epub 2013 Jan 16. Nephrol Dial Transplant. 2013. PMID: 23328709
-
Measures of Urinary Protein and Albumin in the Prediction of Progression of IgA Nephropathy.Clin J Am Soc Nephrol. 2016 Jun 6;11(6):947-955. doi: 10.2215/CJN.10150915. Epub 2016 Mar 29. Clin J Am Soc Nephrol. 2016. PMID: 27026518 Free PMC article.
-
Empiricism or rationalism: how should we measure proteinuria?Ann Clin Biochem. 2013 Jul;50(Pt 4):296-300. doi: 10.1177/0004563212473283. Epub 2013 Jun 20. Ann Clin Biochem. 2013. PMID: 23787260 Review.
-
Chronic kidney disease and measurement of albuminuria or proteinuria: a position statement.Med J Aust. 2012 Aug 20;197(4):224-5. doi: 10.5694/mja11.11468. Med J Aust. 2012. PMID: 22900872
Cited by
-
Body mass index modifies the effect of urinary protein-to-creatinine ratio on chronic kidney disease progression.Int Urol Nephrol. 2024 Jul;56(7):2371-2378. doi: 10.1007/s11255-024-03984-z. Epub 2024 Feb 26. Int Urol Nephrol. 2024. PMID: 38407753
-
Salvianolic Acid A Improves Rat Kidney Injury by Regulating MAPKs and TGF-β1/Smads Signaling Pathways.Molecules. 2023 Apr 21;28(8):3630. doi: 10.3390/molecules28083630. Molecules. 2023. PMID: 37110864 Free PMC article.
-
Influence of guideline adherence and parameter control on the clinical outcomes in patients with diabetic nephropathy.BMJ Open Diabetes Res Care. 2020 Jul;8(1):e001166. doi: 10.1136/bmjdrc-2019-001166. BMJ Open Diabetes Res Care. 2020. PMID: 32675172 Free PMC article.
-
Allograft Function as Endpoint for Clinical Trials in Kidney Transplantation.Transpl Int. 2022 May 20;35:10139. doi: 10.3389/ti.2022.10139. eCollection 2022. Transpl Int. 2022. PMID: 35669976 Free PMC article.
-
Blood Pressure Variability and the Progression of Chronic Kidney Disease: a Systematic Review and Meta-Analysis.J Gen Intern Med. 2023 Apr;38(5):1272-1281. doi: 10.1007/s11606-022-08001-6. Epub 2023 Jan 17. J Gen Intern Med. 2023. PMID: 36650323 Free PMC article.
References
-
- Gansevoort RT, Matsushita K, van der Velde M, Astor BC, Woodward M, Levey AS, de Jong PE, Coresh J, Chronic Kidney Disease Prognosis Consortium Lower estimated GFR and higher albuminuria are associated with adverse kidney outcomes. A collaborative meta-analysis of general and high-risk population cohorts. Kidney Int. 2011;80:93–104. doi: 10.1038/ki.2010.531. - DOI - PMC - PubMed
-
- Astor BC, Matsushita K, Gansevoort RT, van der Velde M, Woodward M, Levey AS, de Jong PE, Coresh J, Consortium P. Lower estimated glomerular filtration rate and higher albuminuria are associated with mortality and end-stage renal disease. A collaborative meta-analysis of kidney disease population cohorts. Kidney Int. 2011;79:1331–1340. doi: 10.1038/ki.2010.550. - DOI - PMC - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO 2012 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Inter Suppl. 2013;3:1–150.
-
- National Kidney Foundation. K/DOQI Clinical Practice Guidelines for Chronic Kidney Disease: evaluation, classification, and stratification. Am J Kidney Dis. 2002;39(suppl 1):S1–S266. - PubMed
-
- National Collaborating Centre for Chronic Conditions. Chronic Kidney Disease (Partial Update). Early identification and management of chronic kidney diseae in adults in primary and secondary care. London: Royal College of Physicians; 2014. p. 1–447.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
