

The origins of breast cancer associated with mammographic density: a testable biological hypothesis
- PMID: 29514672
- PMCID: PMC5842598
- DOI: 10.1186/s13058-018-0941-y
The origins of breast cancer associated with mammographic density: a testable biological hypothesis
Abstract
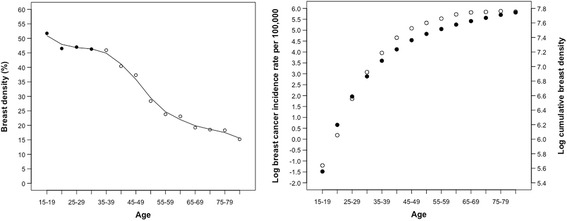
Background: Our purpose is to develop a testable biological hypothesis to explain the known increased risk of breast cancer associated with extensive percent mammographic density (PMD), and to reconcile the apparent paradox that although PMD decreases with increasing age, breast cancer incidence increases.
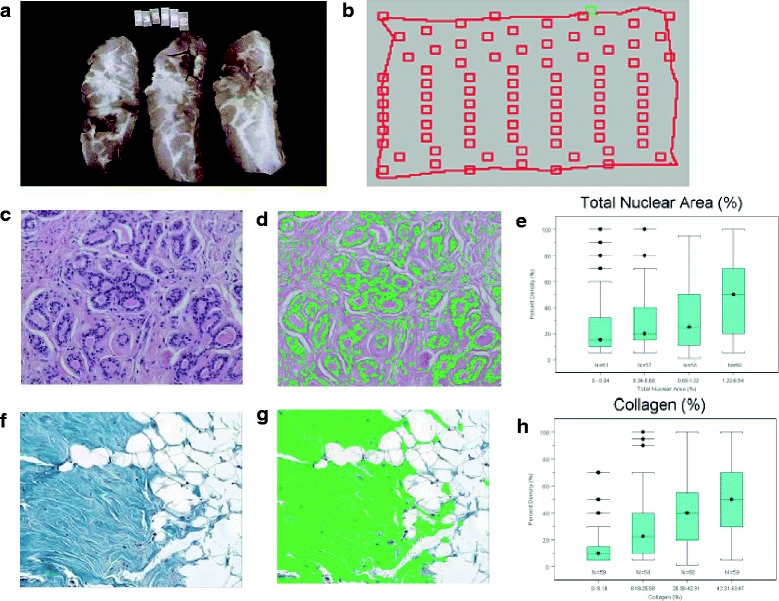
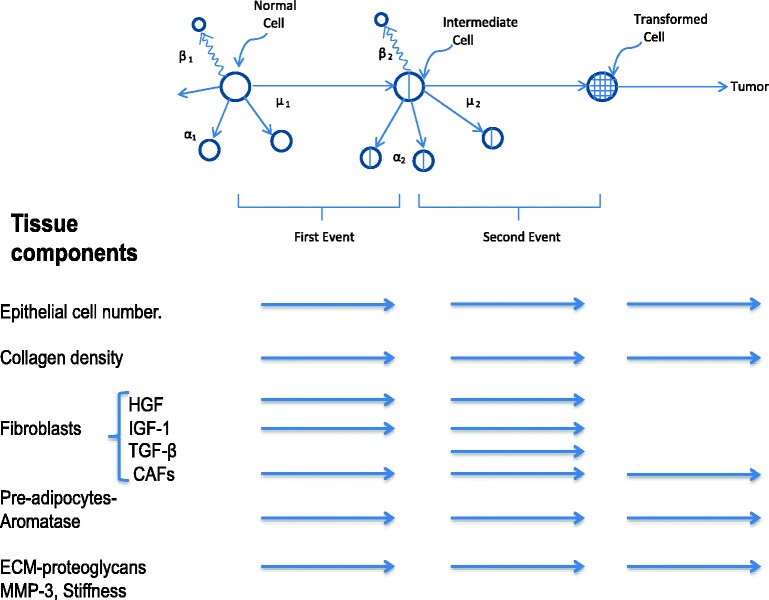
Methods: We used the Moolgavkar model of carcinogenesis as a framework to examine the known biological properties of the breast tissue components associated with PMD that includes epithelium and stroma, in relation to the development of breast cancer. In this model, normal epithelial cells undergo a mutation to become intermediate cells, which, after further mutation, become malignant cells. A clone of such cells grows to become a tumor. The model also incorporates changes with age in the number of susceptible epithelial cells associated with menarche, parity, and menopause. We used measurements of the radiological properties of breast tissue in 4454 healthy subjects aged from 15 to 80+ years to estimate cumulative exposure to PMD (CBD) in the population, and we examined the association of CBD with the age-incidence curve of breast cancer in the population.
Results: Extensive PMD is associated with a greater number of breast epithelial cells, lobules, and fibroblasts, and greater amounts of collagen and extracellular matrix. The known biological properties of these tissue components may, singly or in combination, promote the acquisition of mutations by breast epithelial cells specified by the Moolgavkar model, and the subsequent growth of a clone of malignant cells to form a tumor. We also show that estimated CBD in the population from ages 15 to 80+ years is closely associated with the age-incidence curve of breast cancer in the population.
Conclusions: These findings are consistent with the hypothesis that the biological properties of the breast tissue components associated with PMD increase the probability of the transition of normal epithelium to malignant cells, and that the accumulation of mutations with CBD may influence the age-incidence curve of breast cancer. This hypothesis gives rise to several testable predictions.
Keywords: Breast cancer; Carcinogenesis; Mammographic density; Two-stage model.
Conflict of interest statement
Ethics approval and consent to participate
The data in the section of the manuscript concerned with CBD and the age-specific incidence of breast cancer were obtained in a number of separate studies for which ethics approval was obtained from the University Health Network, Sunnybrook Hospital, and Women’s College Hospital (all in Toronto), and from the Toronto District School Board, the Toronto Catholic District School Board, the York Region District School Board, the York Catholic District School Board, and the mammography screening programs of Ontario and British Columbia.
Consent for publication
All subjects provided signed inform consent.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Bertrand KA, Scott CG, Tamimi RM, Jensen MR, Pankratz VS, Norman AD, Visscher DW, Couch FJ, Shepherd J, Chen YY, et al. Dense and nondense mammographic area and risk of breast cancer by age and tumor characteristics. Cancer Epidemiol Biomarkers Prevent. 2015;24(5):798–809. doi: 10.1158/1055-9965.EPI-14-1136. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
