

Estimated 24-Hour Urinary Sodium and Potassium Excretion in US Adults
- PMID: 29516104
- PMCID: PMC5885845
- DOI: 10.1001/jama.2018.1156
Estimated 24-Hour Urinary Sodium and Potassium Excretion in US Adults
Abstract
Importance: In 2010, the Institute of Medicine (now the National Academy of Medicine) recommended collecting 24-hour urine to estimate US sodium intake because previous studies indicated 90% of sodium consumed was excreted in urine.
Objective: To estimate mean population sodium intake and describe urinary potassium excretion among US adults.
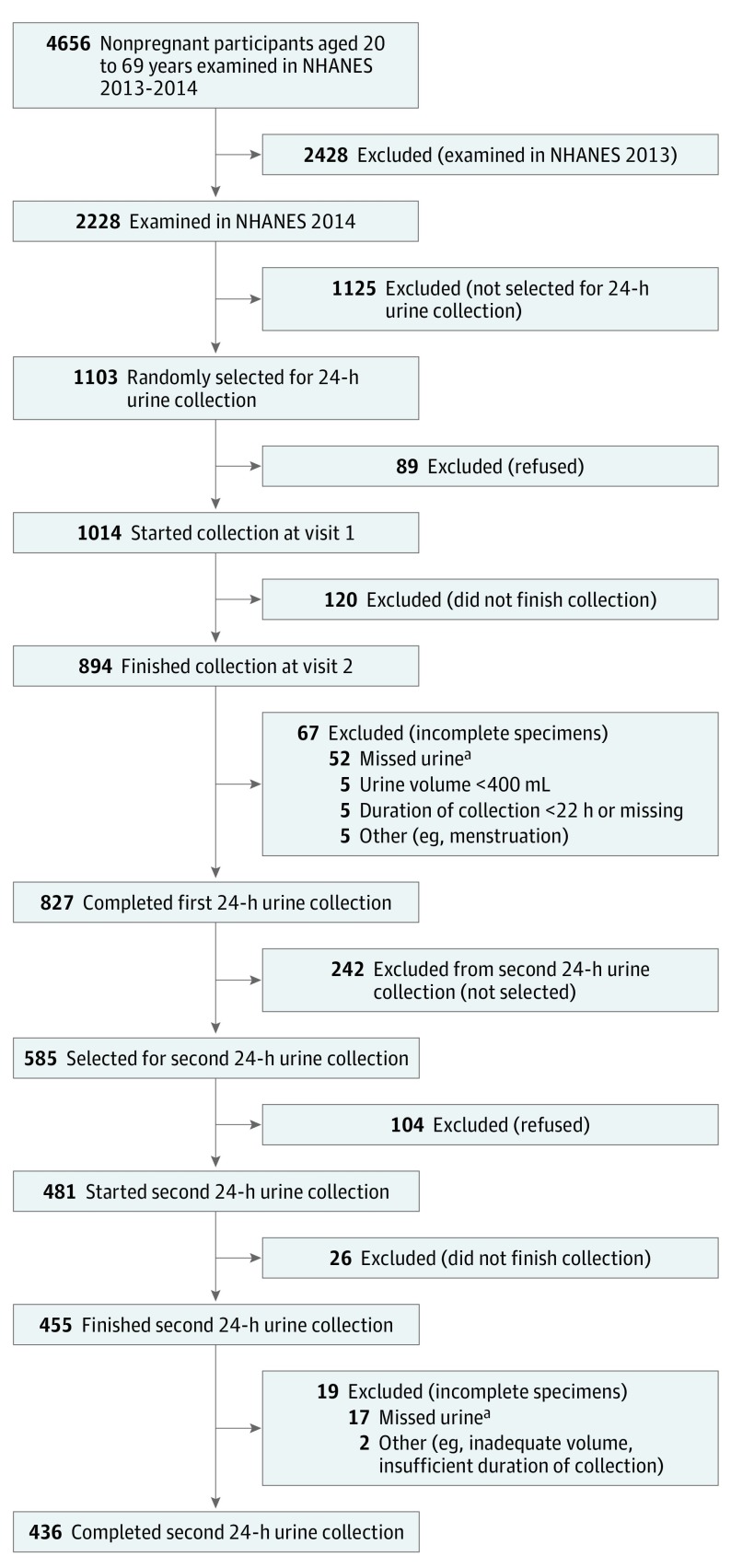
Design, setting, and participants: In a nationally representative cross-sectional survey of the US noninstitutionalized population, 827 of 1103 (75%) randomly selected, nonpregnant participants aged 20 to 69 years in the examination component of the National Health and Nutrition Examination Survey (NHANES) collected at least one 24-hour urine specimen in 2014. The overall survey response rate for the 24-hour urine collection was approximately 50% (75% [24-hour urine component response rate] × 66% [examination component response rate]).
Exposures: 24-hour collection of urine.
Main outcomes and measures: Mean 24-hour urinary sodium and potassium excretion. Weighted national estimates of demographic and health characteristics and mean electrolyte excretion accounting for the complex survey design, selection probabilities, and nonresponse.
Results: The study sample (n = 827) represented a population of whom 48.8% were men; 63.7% were non-Hispanic white, 15.8% Hispanic, 11.9% non-Hispanic black, and 5.6% non-Hispanic Asian; 43.5% had hypertension (according to 2017 hypertension guidelines); and 10.0% reported a diagnosis of diabetes. Overall mean 24-hour urinary sodium excretion was 3608 mg (95% CI, 3414-3803). The overall median was 3320 mg (interquartile range, 2308-4524). In secondary analyses by sex, mean sodium excretion was 4205 mg (95% CI, 3959-4452) in men (n = 421) and 3039 mg (95% CI, 2844-3234) in women (n = 406). By age group, mean sodium excretion was 3699 mg (95% CI, 3449-3949) in adults aged 20 to 44 years (n = 432) and 3507 mg (95% CI, 3266-3748) in adults aged 45 to 69 years (n = 395). Overall mean 24-hour urinary potassium excretion was 2155 mg (95% CI, 2030-2280); by sex, 2399 mg (95% CI, 2253-2545) in men and 1922 mg (95% CI, 1757-2086) in women; and by age, 1986 mg (95% CI, 1878-2094) in adults aged 20 to 44 years and 2343 mg (95% CI, 2151-2534) in adults aged 45 to 69 years.
Conclusions and relevance: In cross-sectional data from a 2014 sample of US adults, estimated mean sodium intake was 3608 mg per day. The findings provide a benchmark for future studies.
Conflict of interest statement
Figures
Comment in
-
Measurements of 24-Hour Urinary Sodium and Potassium Excretion: Importance and Implications.JAMA. 2018 Mar 27;319(12):1201-1202. doi: 10.1001/jama.2018.1153. JAMA. 2018. PMID: 29516102 No abstract available.
-
Sodium Excretion in Population Subgroups.JAMA. 2018 Aug 21;320(7):719-720. doi: 10.1001/jama.2018.8012. JAMA. 2018. PMID: 30140871 No abstract available.
References
-
- He FJ, Li J, Macgregor GA. Effect of longer term modest salt reduction on blood pressure: Cochrane systematic review and meta-analysis of randomised trials. BMJ. 2013;346:f1325. - PubMed
-
- Institute of Medicine Strategies to Reduce Sodium Intake in the United States. Washington, DC: National Academies Press; 2010.
-
- Institute of Medicine Institute of Medicine, Panel on Dietary Reference Intakes for Electrolytes and Water: Dietary Reference Intakes for Water, Potassium Sodium, Chloride, and Sulfate. Washington, DC: National Academies Press; 2005.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
