

18F-Fluorocholine PET/CT in the assessment of primary hyperparathyroidism compared with 99mTc-MIBI or 99mTc-tetrofosmin SPECT/CT: a prospective dual-centre study in 100 patients
- PMID: 29516131
- PMCID: PMC6097754
- DOI: 10.1007/s00259-018-3980-9
18F-Fluorocholine PET/CT in the assessment of primary hyperparathyroidism compared with 99mTc-MIBI or 99mTc-tetrofosmin SPECT/CT: a prospective dual-centre study in 100 patients
Abstract
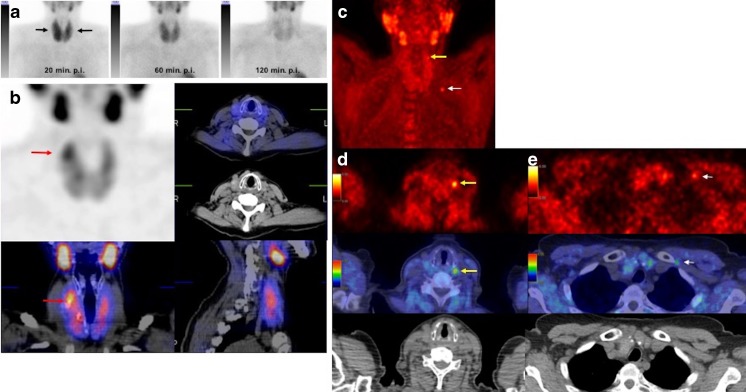
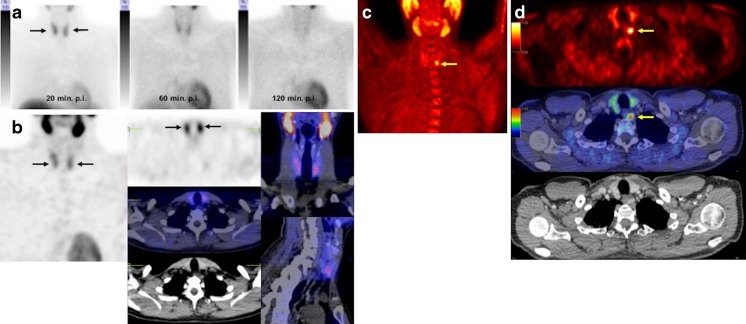
Purpose: In this prospective study we compared the accuracy of 18F-fluorocholine PET/CT with that of 99mTc-MIBI or99mTc-tetrofosmin SPECT/CT in the preoperative detection of parathyroid adenoma in patients with primary hyperparathyroidism. We also assessed the value of semiquantitative parameters in differentiating between parathyroid hyperplasia and adenoma.
Methods: Both 18F-fluorocholine PET/CT and 99mTc-MIBI/tetrofosmin SPECT/CT were performed in 100 consecutive patients with biochemical evidence of primary hyperparathyroidism. At least one abnormal focus on either 18F-fluorocholine or 99mTc-MIBI/tetrofosmin corresponding to a parathyroid gland or ectopic parathyroid tissue was considered as a positive finding. In 76 patients with positive findings on at least one imaging modality, surgical exploration was performed within 6 months, and the results were related to histopathological findings and clinical and laboratory findings at 3-6 months as the standard of truth. In 24 patients, no surgery was performed: in 18 patients with positive imaging findings surgery was refused or considered risky, and in 6 patients imaging was negative. Therefore, data from 82 patients (76 undergoing surgery, 6 without surgery) in whom the standard of truth criteria were met, were used in the final analysis.
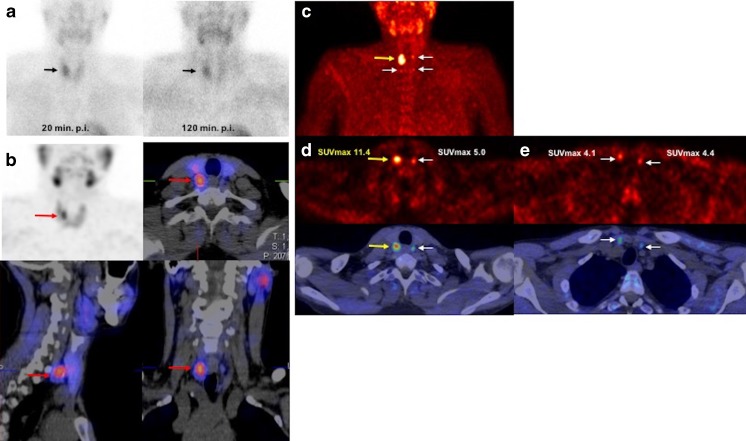
Results: All patients showed biochemical evidence of primary hyperparathyroidism with a mean serum calcium level of 2.78 ± 0.34 mmol/l and parathormone (PTH) level of 196.5 ± 236.4 pg/ml. The study results in 76 patients with verified histopathology and 3 patients with negative imaging findings were analysed. Three of six patients with negative imaging showed normalized serum PTH and calcium levels on laboratory follow-up at 3 and 6 months, and the results were considered true negative. In a patient-based analysis, the detection rate with 18F-fluorocholine PET/CT was 93% (76/82), but was only 61% (50/82) with 99mTc-MIBI/tetrofosmin SPECT/CT. In a lesion-based analysis, the sensitivity, specificity, positive predictive value, negative predictive value and overall accuracy of 18F-fluorocholine PET/CT in the detection of parathyroid adenoma were 93.7%, 96.0%, 90.2%, 97.4% and 95.3%, respectively, and of 99mTc-MIBI/tetrofosmin SPECT/CT were 60.8%, 98.5%, 94.1%, 86.3% and 87.7%, respectively. Although 18F-fluorocholine PET-positive adenomatous lesions showed higher SUVmax values than the hyperplastic glands (6.80 ± 3.78 vs. 4.53 ± 0.40) in the semiquantitative analysis, the difference was not significant (p = 0.236). The mean size (measured as the length of the greatest dimension) and weight of adenomas were 15.9 ± 7.6 mm (median 15 mm, range 1-40 mm) and 1.71 ± 1.86 g (median 1 g, range: 0.25-9 g), respectively. Among the analysed parameters including serum calcium and PTH and the size and weight of parathyroid adenomas, size was significantly different between patients with negative 99mTc-MIBI/tetrofosmin SPECT/CT and those with positive 99mTc-MIBI/tetrofosmin SPECT/CT (mean size 13.4 ± 7.6 mm vs. 16.9 ± 7.4 mm, respectively; p = 0.042).
Conclusion: In this prospective study, 18F-fluorocholine PET/CT showed promise as a functional imaging modality, being clearly superior to 99mTc-MIBI/tetrofosmin SPECT/CT, especially in the detection and localization of small parathyroid adenomas in patients with primary hyperparathyroidism. SUVmax was higher in parathyroid adenomas than in hyperplasia. However, further evaluation of this modality is needed.
Keywords: 18F-Fluorocholine PET/CT; 99mTc-MIBI; 99mTc-Tetrofosmin; Primary hyperparathyroidism; SPECT/CT.
Conflict of interest statement
Conflicts of interest
None.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Figures
References
-
- Taniegra ED. Hyperparathyroidism. Am Fam Physician. 2004;69:333–339. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
