

Detection of surgical margins in oral cavity cancer: the role of dynamic optical contrast imaging
- PMID: 29517537
- PMCID: PMC5846197
- DOI: 10.1097/MOO.0000000000000444
Detection of surgical margins in oral cavity cancer: the role of dynamic optical contrast imaging
Abstract
Purpose of review: The quantity of tissue removed during an oncologic surgical procedure is not standardized and there are numerous reports of local recurrence despite histologically adequate resection margins. The oral cavity is one of the sites in the head and neck with high chances of recurrence following negative margins. To address this need, this article reviews the recent applications of Dynamic Optical Contrast Imaging (DOCI) towards both oral screening and the intraoperative evaluation of tumor margins in head and neck surgery.
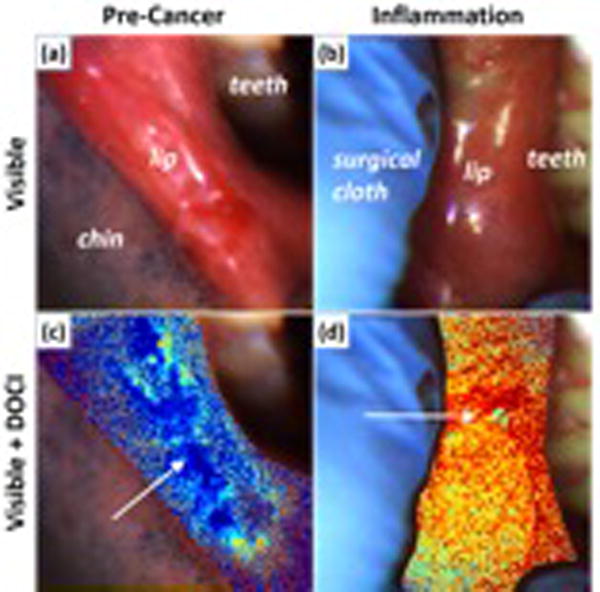
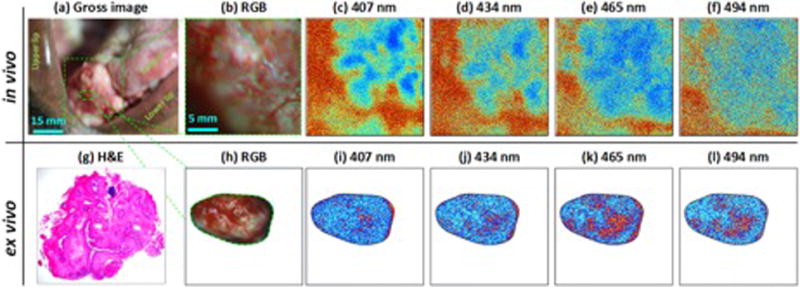
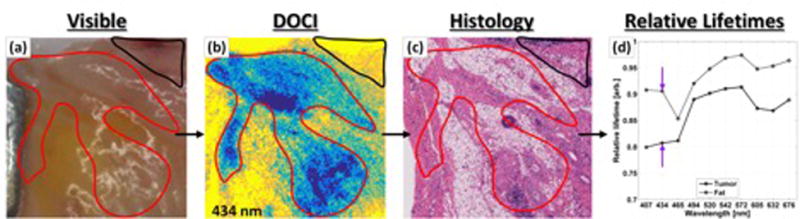
Recent findings: Human ex-vivo and in-vivo trials suggest DOCI is well tolerated, low-cost, and sensitive for differentiating cancerous from normal tissues throughout the head and neck, in addition to the oral cavity. Ex-vivo imaging of OSCC specimens generated histologically verified image contrast. Furthermore, in-vivo intraoperative results demonstrate significant potential for image-guided detection and resection of oral cavity squamous cell carcinoma (OSCC).
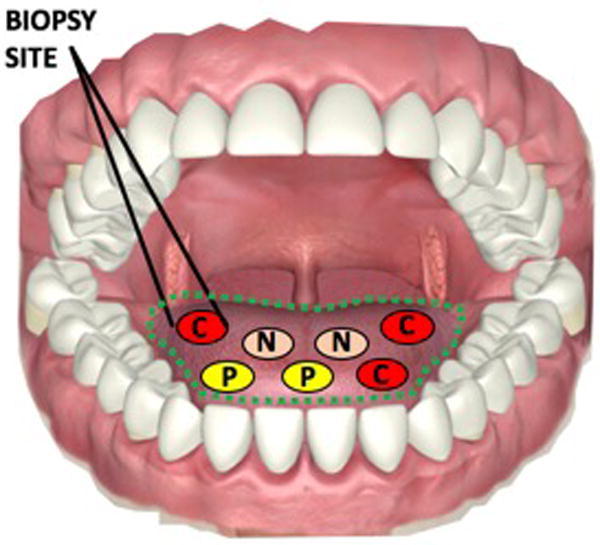
Summary: DOCI augments tissue contrast and may enable surgeons to clinically screen patients for oral cancer, make histologic evaluations in vivo with fewer unnecessary biopsies, delineate clinical margins for tumor resection, provide guidance in the choice of biopsy sites, and preserve healthy tissue to increase the postoperative functionality and quality of life of the patient.
Conflict of interest statement
None.
Figures
References
-
- Forastiere A, Koch W, Trotti A, Sidransky D. Head and neck cancer. N Engl J Med. 2001;345:1890–1900. - PubMed
-
- Carvalho AL, K LP. Influence of time delay and clinical upstaging in the prognosis of head and neck cancer. Oral Oncol. 37:94–98. - PubMed
-
- McGurk M, Chan C, Jones J, O’regan E, Sherriff M. Delay in diagnosis and its effect on outcome in head and neck cancer. Br J Oral Maxillofac Surg. 43:281–284. - PubMed
-
- Lang K, Menzin J, Earle CC, Jacobson J, Hsu M-A. The economic cost of squamous cell cancer of the head and neck: findings from linked SEER-Medicare data. Arch Otolaryngol Neck Surg. 2004;130:1269–1275. - PubMed
-
- Lee JM, Turini M, Botteman MF, Stephens JM, Pashos CL. Economic burden of head and neck cancer. Eur J Heal Econ Former HEPAC. 2004;5:70–80. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials