

Minimal invasive nonfusion technique for the treatment of noncontiguous lumbar burst fractures in young age patient: A case report
- PMID: 29517657
- PMCID: PMC5882417
- DOI: 10.1097/MD.0000000000010009
Minimal invasive nonfusion technique for the treatment of noncontiguous lumbar burst fractures in young age patient: A case report
Abstract
Rationale: In the treatment of noncontiguous lumbar burst fractures, there still remains controversy over proper surgical procedures.
Patient concerns: A 19-year-old female patient visited our hospital after fall down from 3 m high.
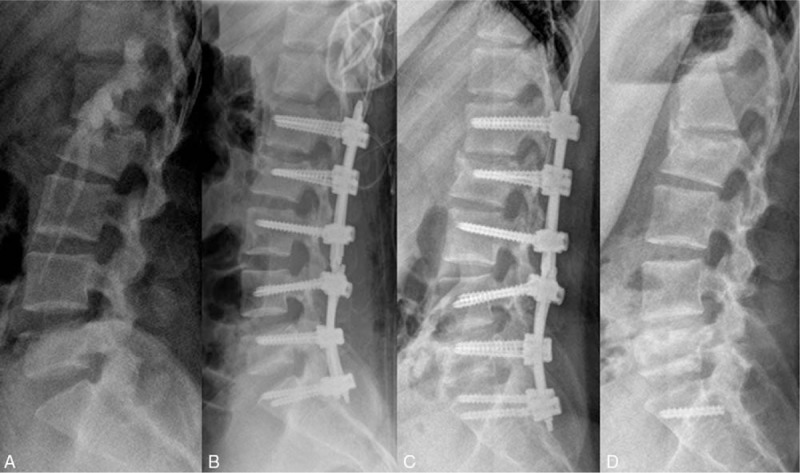
Diagnoses: Initial neurologic examination revealed an incomplete spinal cord injury characterized by hypoesthesia and motor grade of 2 below the L2 segment. Lumbar computed tomography and magnetic resonance imaging demonstrated L2 and L5 burst fractures severely obliterating the spinal canal.
Interventions: She underwent emergent PSSPSF at L1-2-3 and L4-5-S1 following bilateral L1 and L4 laminotomy with reduction of bony fragments by tapping method.
Outcomes: She was gradually recovered and able to walk with assistance two weeks after surgery. Removal of implants was performed at 12 months after surgery. Follow-up radiography showed well-preserved segmental motion and adequate decompressed spinal canal with fused fractured bony fragment. She returned to her normal daily activities without any neurologic deficits and pain.
Lessons: Noncontiguous burst fracture of the lumbar spine is an unusual injury. For the adequate management in patient with neurologic deficit, reduction of the fractured body and stabilization of vertebral column is necessary. It is also important to preserve the segmental motion in young age patients. From that point of view, temporary PSSPSF with spinal canal decompression is considered as minimal invasive surgery with significant low morbidity, providing stability with motion saving and good clinical outcome.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures


References
-
- Bensch FV, Koivikko MP, Kiuru MJ, et al. The incidence and distribution of burst fractures. Emerg Radiol 2006;12:124–9. - PubMed
-
- Kaneda K, Taneichi H, Abumi K, et al. Anterior decompression and stabilization with the Kaneda device for thoracolumbar burst fractures associated with neurological deficits. J Bone Joint Surg Am 1997;79:69–83. - PubMed
-
- Sasso RC, Best NM, Reilly TM, et al. Anterior-only stabilization of three-column thoracolumbar injuries. J Spinal Disord Tech 2005;18:S7–14. - PubMed
-
- Waqar M, Van-Popta D, Barone DG, et al. Short versus long-segment posterior fixation in the treatment of thoracolumbar junction fractures: a comparison of outcomes. Br J Neurosurg 2016;31:1–4. - PubMed
-
- Wood KB, Li W, Lebl DR, et al. Management of thoracolumbar spine fractures. Spine J 2014;14:145–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
