

Hemichorea after hyperglycemia correction: A case report and a short review of hyperglycemia-related hemichorea at the euglycemic state
- PMID: 29517669
- PMCID: PMC5882440
- DOI: 10.1097/MD.0000000000010076
Hemichorea after hyperglycemia correction: A case report and a short review of hyperglycemia-related hemichorea at the euglycemic state
Abstract
Rationale: Hyperglycemic hemichorea tends to affect elderly patients with type 2 diabetes, women, and the Asian population. The onset of involuntary movement typically occurs at the hyperglycemic state and subsides at the euglycemic state. In this report, we present an unusual case that developed delayed-onset hemichorea after hyperglycemia correction.
Patient concerns: A 70-year-old man was admitted to neurology ward with symptoms of subacute dizziness. Hyperglycemia and high level ketone body was incidentally noted. Hemichorea occurred in his left limbs 2 days after hyperglycemia correction.
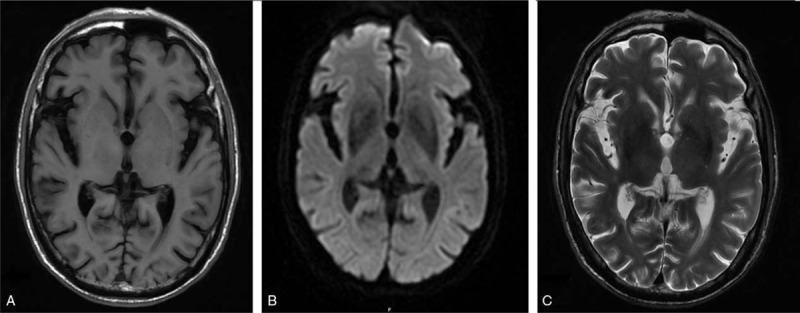
Diagnoses: Patient remained conscious, and no other focal neurological deficits were noted while hemichorea occurred. Blood test revealed no contributory cause. Brain magnetic resonance imaging revealed no lesions in the putamen or subthalamus. A diagnosis of probable hyperglycemia-related hemichorea was made.
Interventions: Haloperidol (2 mg, 3 times per day) was prescribed.
Outcomes: Hemichorea improved gradually before discharge and resolved 4 months later.
Lessons: Differential diagnosis of hemichorea should include delayed-onset hemichorea after hyperglycemia correction.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Oh SH, Lee KY, Im JH, et al. Chorea associated with non-ketotic hyperglycemia and hyperintensity basal ganglia lesion on T1-weighted brain MRI study: a meta-analysis of 53 cases including four present cases. J Neurol Sci 2002;200:57–62. - PubMed
-
- Taboada GF, Lima GA, Castro JE, et al. Dyskinesia associated with hyperglycemia and basal ganglia hyperintensity: report of a rare diabetic complication. Metab Brain Dis 2013;28:107–10. - PubMed
-
- Branca D, Gervasio O, Le Piane E, et al. Chorea induced by non-ketotic hyperglycaemia: a case report. Neurol Sci 2005;26:275–7. - PubMed
-
- Lai PH, Chen PC, Chang MH, et al. In vivo proton MR spectroscopy of chorea-ballismus in diabetes mellitus. Neuroradiology 2001;43:525–31. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
