

ICU mortality following ICU-acquired primary bloodstream infections according to the type of pathogen: A prospective cohort study in 937 Germany ICUs (2006-2015)
- PMID: 29518133
- PMCID: PMC5843291
- DOI: 10.1371/journal.pone.0194210
ICU mortality following ICU-acquired primary bloodstream infections according to the type of pathogen: A prospective cohort study in 937 Germany ICUs (2006-2015)
Abstract
Objective: Mortality due to intensive care unit (ICU) acquired primary blood stream infections (PBSI) is related primarily to patient co-morbidities, types of pathogens and quality of care. The objective of this study is to determine the impact of various types of pathogen on ICU mortality.
Methods: Data from the German National Nosocomial Infection Surveillance System of patients with PBSI from 2006 to 2015 was used for this analysis. A BSI is primary when the pathogen recognized is not related to an infection on another site. Only mono-microbial infections stratified into the 13 pathogens most frequently causing PBSI were considered. Univariate and multivariate risk factor analyses were performed using the following risk factors: Sex, age, length of stay, device use, time until onset of PBSI, type and size of hospital, type of ICU and type of pathogen. ICU mortality following S.aureus PBSI was used as the reference value.
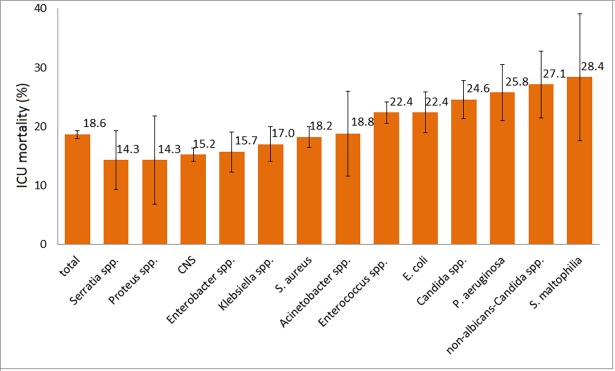
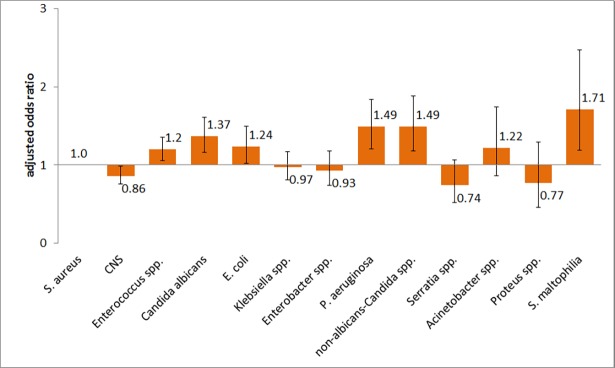
Results: A total of 4,556,360 patients with 16,978,882 patient days from 937 ICUs were considered in the analysis. Of 14,626 PBSI in total, 12,745 mono-microbial PBSI were included. The ICU mortality was 18.6%. Compared with S.aureus and adjusted by age, sex and type of ICU, S.maltophilia was associated with significantly higher ICU mortality (OR 1.71; 95%CI 1.19-2.47) as followed by Enterococci (OR 1.20; 95%CI 1.06-1.36), E.coli (OR 1.24; 95%CI 1.02-1.49), C.albicans (OR 1.37; 95%CI 1.16-1.61), non albicans Candida spp. (OR 1.49; 95%CI 1.18-1.88) and P.aeruginosa (OR 1.49; 95%CI 1.21-1.84). Coagulase negative Staphylococci were associated with significant lower ICU mortality (OR 0.86; 95%CI 0.75-0.99).
Conclusion: Because of the limitation of the study in adjusting for severity of illness and appropriateness of therapy, the differences between the pathogens may not only be explained by differences in virulence, but may reflect the prognosis after receiving the microbiological results and may therefore be useful for intensive care physicians.
Conflict of interest statement
Figures
References
-
- Shorr A. Review of studies of the impact on Gram-negative bacterial resistance on outcomes in the intensive care unit. Crit Care Med. 2009;37:1463–39. doi: 10.1097/CCM.0b013e31819ced02 - DOI - PubMed
-
- Lemos E, de la Hoz F, Einarson T, McGhan W, Quevedo E, Castañeda C, et al. Carbapenem resistance and mortality in patients with Acinetobacter baumannii infection: systematic review and meta-analysis. Clin Microbiol Infect 2014;20:416–23. doi: 10.1111/1469-0691.12363 - DOI - PubMed
-
- Ani C, Farshidpanah S, Bellinghausen Stewart A, Nguyen H. Variations in organism-specific severe sepsis mortality in the United States: 1999–2008. Crit Care Med. 2015;43:65–77. doi: 10.1097/CCM.0000000000000555 - DOI - PubMed
-
- Prowle J, Echeverri J, Ligabo E, Sherry N, Taori G, Crozier T, et al. Acquired bloodstream infection in the intensive care unit: incidence and attributable mortality. Crit Care. 2011;15(2):R100 doi: 10.1186/cc10114 - DOI - PMC - PubMed
-
- Lambert M, Suetens C, Savey A, Palomar M, Hiesmayr M, Morales I, et al. Clinical outcomes of health-care-associated infections and antimicrobial resistance in patients admitted to European intensive-care units: a cohort study. Lancet Infect Dis 2011;11:30–8. doi: 10.1016/S1473-3099(10)70258-9 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
