

Sex, race, and insurance status differences in hospital treatment and outcomes following out-of-hospital cardiac arrest
- PMID: 29518439
- PMCID: PMC5899667
- DOI: 10.1016/j.resuscitation.2018.02.027
Sex, race, and insurance status differences in hospital treatment and outcomes following out-of-hospital cardiac arrest
Abstract
Background: Sex, race, and insurance status are associated with treatment and outcomes in several cardiovascular diseases. These disparities, however, have not been well-studied in out-of-hospital cardiac arrest (OHCA).
Objective: Our objective was to evaluate the association of patient sex, race, and insurance status with hospital treatments and outcomes following OHCA.
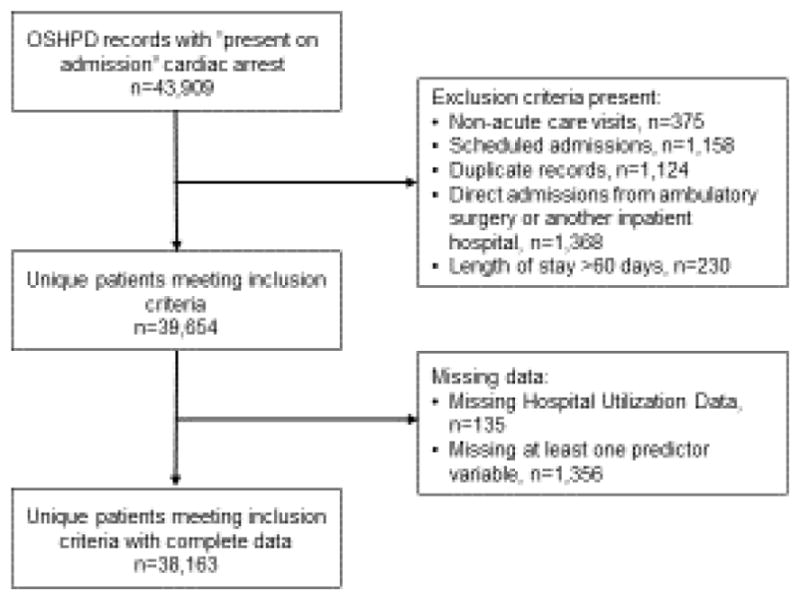
Methods: We studied adult patients in the 2011-2015 California Office of Statewide Health Planning and Development (OSHPD) Patient Discharge Database with a "present on admission" diagnosis of cardiac arrest (ICD-9-CM 427.5). Insurance status was classified as private, Medicare, and Medi-Cal/government/self-pay. Our primary outcome was good neurologic recovery at hospital discharge, which was determined by discharge disposition. Secondary outcomes were survival to hospital discharge, treatment at a 24/7 percutaneous coronary intervention (PCI) center, "do not resuscitate" orders within 24 h of admission, and cardiac catheterization during hospitalization. Data were analyzed with hierarchical multiple logistic regression models.
Results: We studied 38,163 patients in the OSHPD database. Female sex, non-white race, and Medicare insurance status were independently associated with worse neurologic recovery [OR 0.94 (0.89-0.98), 0.93 (0.88-0.98), and 0.85 (0.79-0.91), respectively], lower rates of treatment at a 24/7 PCI center [OR 0.89 (0.85-0.93), 0.88 (0.85-0.93), and 0.87 (0.82-0.94), respectively], and lower rates of cardiac catheterization [OR 0.61 (0.57-0.65), 0.90 (0.84-0.97), and 0.44 (0.40-0.48), respectively]. Female sex, white race, and Medicare insurance were associated with DNR orders within 24 h of admission [OR 1.16 (1.10-1.23), 1.14 (1.07-1.21), and 1.25 (1.15-1.36), respectively].
Conclusions: Sex, race, and insurance status were independently associated with post-arrest care interventions, patient outcomes and treatment at a 24/7 PCI center. More studies are needed to fully understand the causes and implications of these disparities.
Keywords: Cardiac arrest; Disparities; Sex differences.
Copyright © 2018 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
References
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart Disease and Stroke Statistics-2016 Update: A Report from the American Heart Association. Circulation. 2016;133:e38–360. - PubMed
-
- Richardson DK, Zive D, Daya M, et al. The Impact of Early Do Not Resuscitate (DNR) Orders on Patient Care and Outcomes Following Resuscitation from out of Hospital Cardiac Arrest. Resuscitation. 2013;84:483–7. - PubMed
-
- Hagihara A, Onozuka D, Ono J, et al. Age X Gender Interaction Effect on Resuscitation Outcomes in Patients with out-of-Hospital Cardiac Arrest. Am J Cardiol. 2017 - PubMed
-
- Eid SM, Abougergi MS, Albaeni A, et al. Survival, Expenditure and Disposition in Patients Following out-of-Hospital Cardiac Arrest: 1995–2013. Resuscitation. 2017;113:13–20. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
