

10-Year Resource Utilization and Costs for Cardiovascular Care
- PMID: 29519347
- PMCID: PMC5846485
- DOI: 10.1016/j.jacc.2017.12.064
10-Year Resource Utilization and Costs for Cardiovascular Care
Abstract
Background: Cardiovascular disease (CVD) imparts a heavy economic burden on the U.S. health care system. Evidence regarding the long-term costs after comprehensive CVD screening is limited.
Objectives: This study calculated 10-year health care costs for 6,814 asymptomatic participants enrolled in MESA (Multi-Ethnic Study of Atherosclerosis), a registry sponsored by the National Heart, Lung, and Blood Institute, National Institutes of Health.
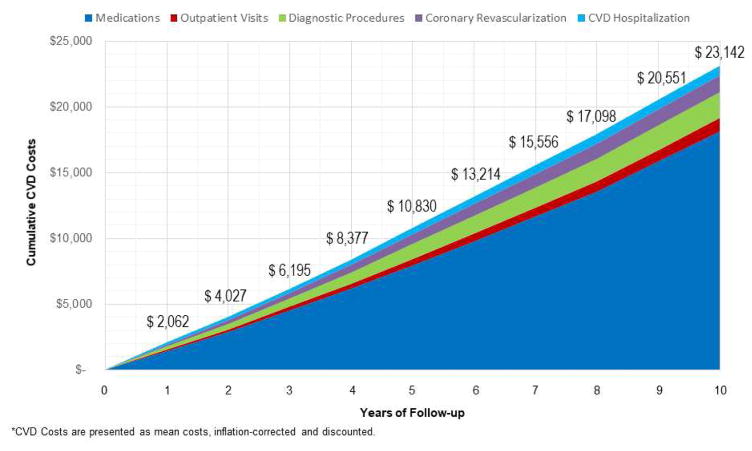
Methods: Cumulative 10-year costs for CVD medications, office visits, diagnostic procedures, coronary revascularization, and hospitalizations were calculated from detailed follow-up data. Costs were derived by using Medicare nationwide and zip code-specific costs, inflation corrected, discounted at 3% per year, and presented in 2014 U.S. dollars.
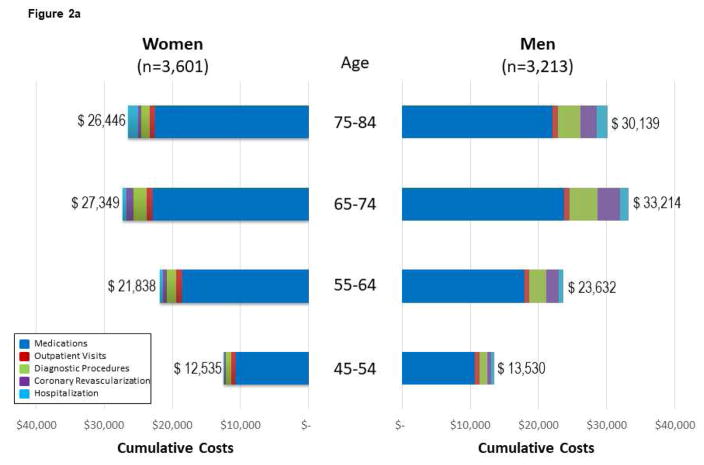
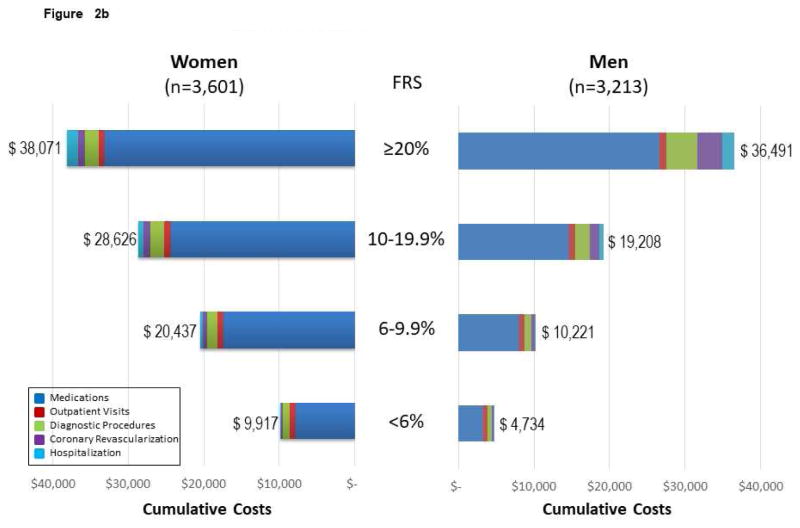
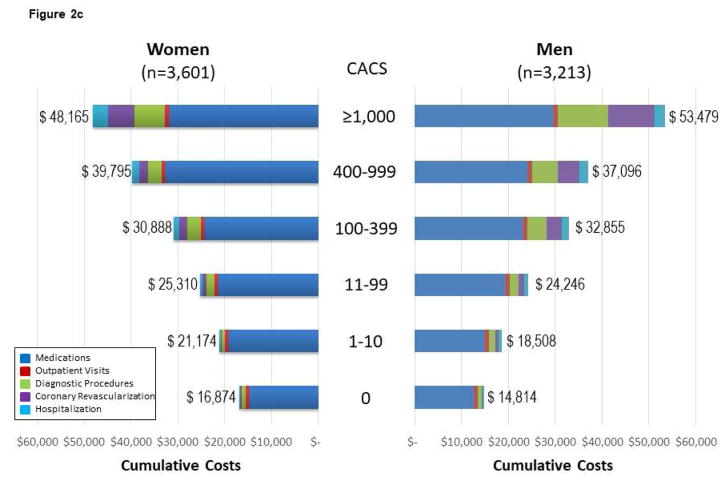
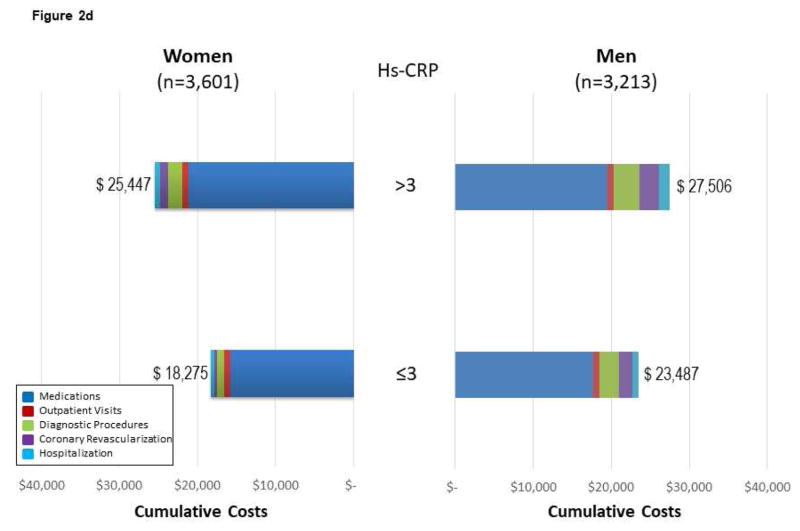
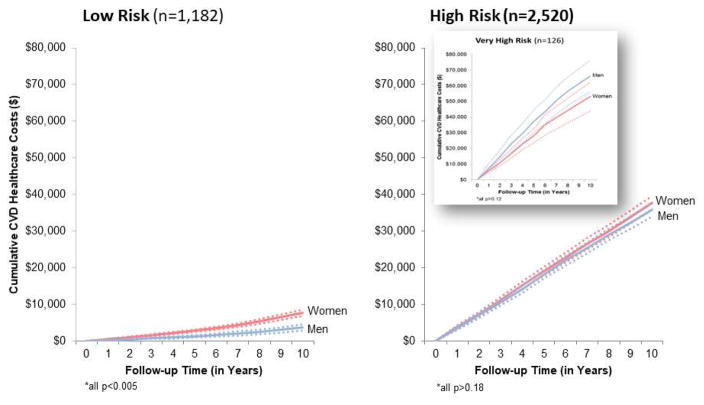
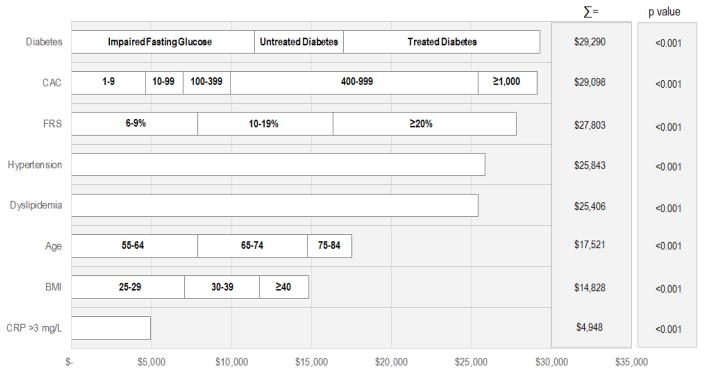
Results: Risk factor prevalence increased dramatically and, by 10 years, diabetes, hypertension, and dyslipidemia was reported in 19%, 57%, and 53%, respectively. Self-reported symptoms (i.e., chest pain or shortness of breath) were common (approximately 40% of enrollees). At 10 years, approximately one-third of enrollees reported having an echocardiogram or exercise test, whereas 7% underwent invasive coronary angiography. These utilization patterns resulted in 10-year health care costs of $23,142. The largest proportion of costs was associated with CVD medication use (78%). Approximately $2 of every $10 were spent for outpatient visits and diagnostic testing among the elderly, obese, those with a high-sensitivity C-reactive protein level >3 mg/l, or coronary artery calcium score (CACS) ≥400. Costs varied widely from <$7,700 for low-risk (Framingham risk score <6%, 0 CACS, and normal glucose measurements at baseline) to >$35,800 for high-risk (persons with diabetes, Framingham risk score ≥20%, or CACS ≥400) subgroups. Among high-risk enrollees, CVD costs accounted for $74 million of the $155 million consumed by MESA participants.
Conclusions: Longitudinal patterns of health care resource use after screening revealed new evidence on the economic burden of treatment and testing patterns not previously reported. Maintenance of a healthy population has the potential to markedly reduce the economic burden of CVD among asymptomatic individuals.
Keywords: asymptomatic; cardiovascular disease screening; economics; long-term follow-up.
Copyright © 2018 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Building the Economic Case for Investment in Cardiovascular Prevention.J Am Coll Cardiol. 2018 Mar 13;71(10):1090-1093. doi: 10.1016/j.jacc.2018.01.022. J Am Coll Cardiol. 2018. PMID: 29519348 No abstract available.
-
Cost of cardiovascular disease prevention: towards economic evaluations in prevention programs.Ann Transl Med. 2020 Apr;8(7):512. doi: 10.21037/atm.2020.01.20. Ann Transl Med. 2020. PMID: 32395556 Free PMC article. No abstract available.
References
-
- Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. 2011;123:933–44. - PubMed
-
- Benjamin EJ, Blaha MJ, Chiuve SE, et al. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics-2017 update: a report from the American Heart Association [Published corrections appear in Circulation 2017;135:e646 and Circulation. 2017;136:e196] Circulation. 2017;135:e146–e603. - PMC - PubMed
-
- Fihn SD, Gardin JM, Abrams J, et al. 2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS Guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, and the American College of Physicians, American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J Am Coll Cardiol. 2012;60:e44–e164. - PubMed
-
- Curry SJ, Byers T, Hewitt M, editors. Fulfilling the Potential of Cancer Prevention and Early Detection. National Academies Press; Washington, DC: 2003. Available at: https://doi.org/10.17226/10263. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
