

Single-Molecule Counting of High-Sensitivity Troponin I in Patients Referred for Diagnostic Angiography: Results From the CASABLANCA (Catheter Sampled Blood Archive in Cardiovascular Diseases) Study
- PMID: 29519811
- PMCID: PMC5907559
- DOI: 10.1161/JAHA.117.007975
Single-Molecule Counting of High-Sensitivity Troponin I in Patients Referred for Diagnostic Angiography: Results From the CASABLANCA (Catheter Sampled Blood Archive in Cardiovascular Diseases) Study
Abstract
Background: The meaning of high-sensitivity troponin I (hsTnI) concentrations in patients without acute myocardial infarction (MI) requires clarity. We hypothesized that among patients referred for diagnostic coronary angiography without acute MI, hsTnI concentrations would correlate with prevalent coronary artery disease (CAD) and predict incident cardiovascular events and mortality.
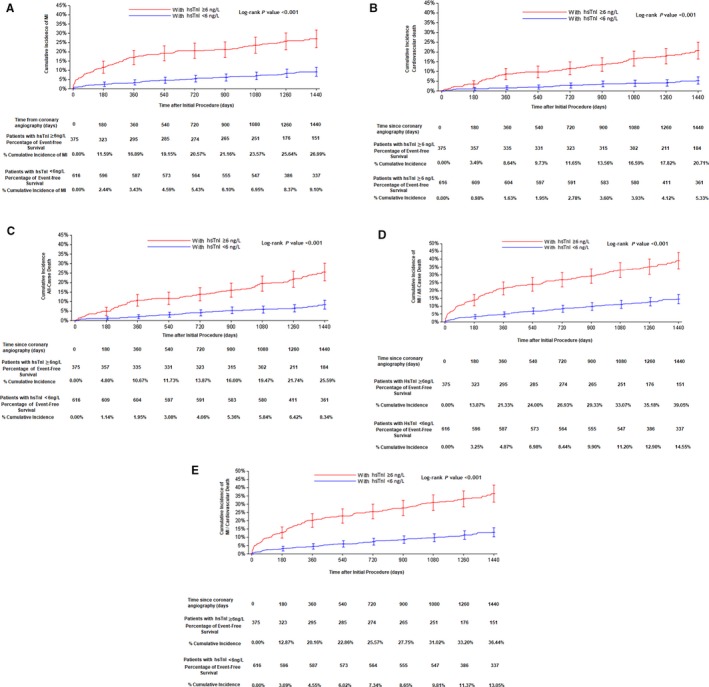
Methods and results: We measured hsTnI using a single-molecule counting assay (99th percentile, 6 ng/L) in samples from 991 patients obtained at the time of angiography. Concentrations of hsTnI were assessed relative to the severity of CAD and prognosis during mean follow-up of 3.7 years. Median hsTnI concentration was 4.19 ng/L; 38% of patients had hsTnI concentrations ≥99th percentile. Across increasing hsTnI quartiles, patients had higher prevalence of angiographic CAD; in multivariate models, hsTnI ≥99th percentile independently predicted obstructive CAD (odds ratio: 2.57; P<0.001) and incident MI (hazard ratio [HR]: 2.68; P<0.001), cardiovascular death (HR: 2.29; P=0.001), and all-cause death (HR: 1.84; P=0.004). In those with >70% coronary stenosis, hsTnI ≥99th percentile independently predicted incident MI (HR: 1.87; P=0.01), cardiovascular mortality (HR: 2.74; P=0.001), and the composite end point of MI and all-cause death (HR: 2.06; P<0.001). In participants with coronary stenosis <70%, hsTnI ≥99th percentile even more strongly predicted incident MI (HR: 8.41; P<0.001), cardiovascular mortality (HR: 3.60; P=0.03), and the composite end point of MI and all-cause death (HR: 3.62; P<0.001).
Conclusions: In a large prospective cohort of patients who were free of prevalent MI and undergoing diagnostic coronary angiography, hsTnI concentrations were associated with higher prevalence of CAD and predicted incident MI, cardiovascular death, and all-cause death.
Clinical trial registration: URL: http://www.clinicaltrials.gov. Unique identifier: NCT00842868.
Keywords: biomarkers; coronary artery disease; high‐sensitivity; troponin.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures

References
-
- Steg PG, Bhatt DL, Wilson PW, D'Agostino R Sr, Ohman EM, Rother J, Liau CS, Hirsch AT, Mas JL, Ikeda Y, Pencina MJ, Goto S. One‐year cardiovascular event rates in outpatients with atherothrombosis. JAMA. 2007;297:1197–1206. - PubMed
-
- Kragelund C, Grønning B, Køber L, Hildebrandt P, Steffensen R. N‐terminal pro‐B‐type natriuretic peptide and long‐term mortality in stable coronary heart disease. N Engl J Med. 2005;352:666–675. - PubMed
-
- Danesh J, Wheeler JG, Hirschfield GM, Eda S, Eiriksdottir G, Rumley A, Lowe GDO, Pepys MB, Gudnason V. C‐reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med. 2004;350:1387–1397. - PubMed
-
- Sabatine MS, Morrow DA, Jablonski KA, Rice MM, Warnica JW, Domanski MJ, Hsia J, Gersh BJ, Rifai N, Ridker PM, Pfeffer MA, Braunwald E. Prognostic significance of the Centers for Disease Control/American Heart Association high‐sensitivity C‐reactive protein cut points for cardiovascular and other outcomes in patients with stable coronary artery disease. Circulation. 2007;115:1528–1536. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
