

Trends in Hospitalizations and Survival of Acute Decompensated Heart Failure in Four US Communities (2005-2014): ARIC Study Community Surveillance
- PMID: 29519849
- PMCID: PMC6030442
- DOI: 10.1161/CIRCULATIONAHA.117.027551
Trends in Hospitalizations and Survival of Acute Decompensated Heart Failure in Four US Communities (2005-2014): ARIC Study Community Surveillance
Abstract
Background: Community trends of acute decompensated heart failure (ADHF) in diverse populations may differ by race and sex.
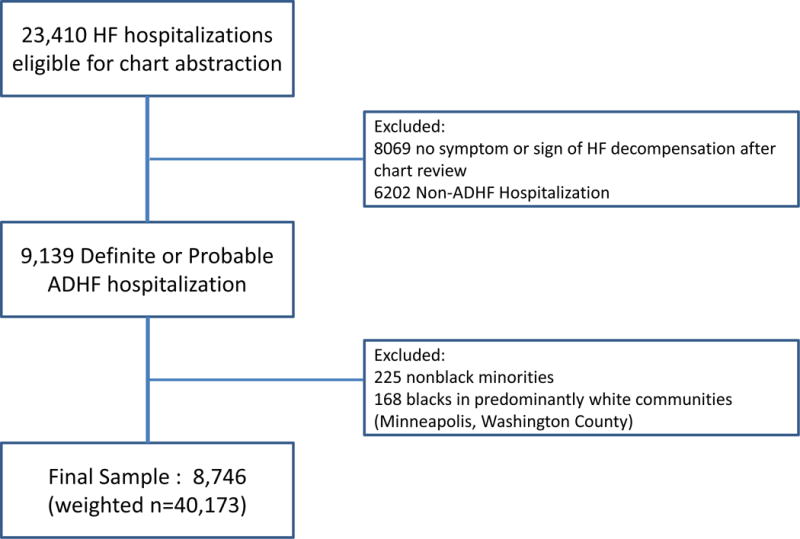
Methods: The ARIC study (Atherosclerosis Risk in Communities) sampled heart failure-related hospitalizations (≥55 years of age) in 4 US communities from 2005 to 2014 using International Classification of Diseases, Ninth Revision, Clinical Modification codes. ADHF hospitalizations were validated by standardized physician review and computer algorithm, yielding 40 173 events after accounting for sampling design (unweighted n=8746).
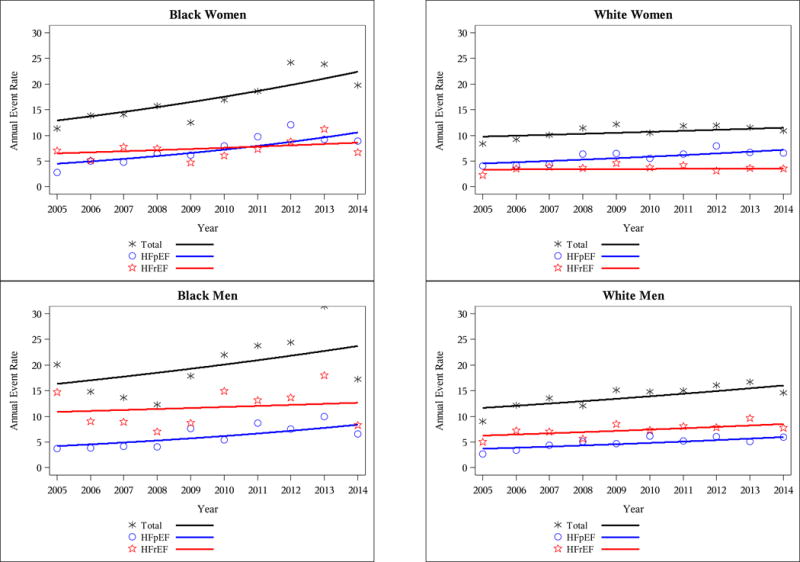
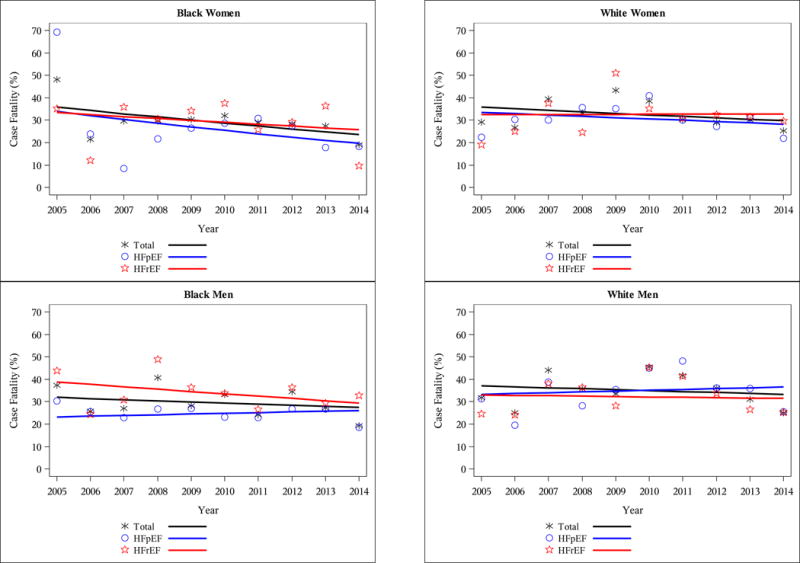
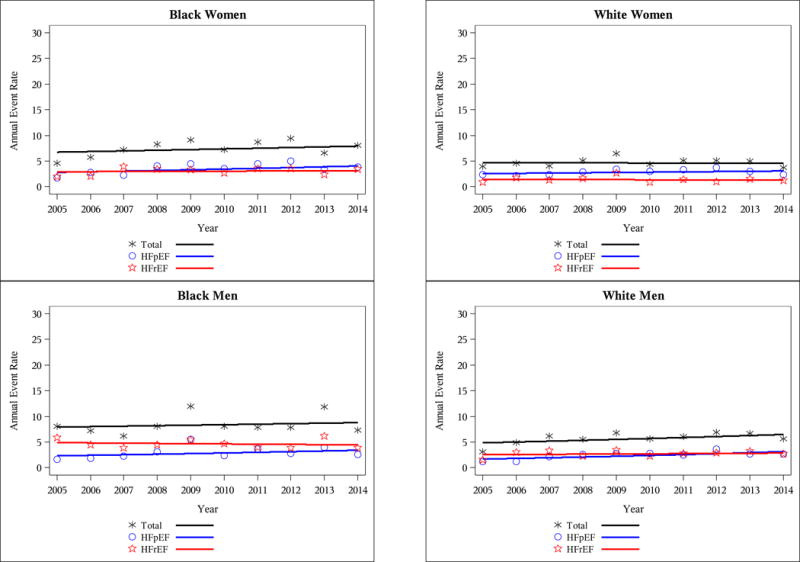
Results: Of the ADHF hospitalizations, 50% had reduced ejection fraction, and 39% had preserved EF (HFpEF). HF with reduced ejection fraction was more common in black men and white men, whereas HFpEF was most common in white women. Average age-adjusted rates of ADHF were highest in blacks (38.1 per 1000 black men, 30.5 per 1000 black women), with rates differing by HF type and sex. ADHF rates increased over the 10 years (average annual percentage change: black women +4.3%, black men +3.7%, white women +1.9%, white men +2.6%), mostly reflecting more acute HFpEF. Age-adjusted 28-day and 1-year case fatality proportions were ≈10% and 30%, respectively, similar across race-sex groups and HF types. Only blacks showed decreased 1-year mortality over time (average annual percentage change: black women -5.4%, black men -4.6%), with rates differing by HF type (average annual percentage change: black women HFpEF -7.1%, black men HF with reduced ejection fraction -4.7%).
Conclusions: Between 2005 and 2014, trends in ADHF hospitalizations increased in 4 US communities, primarily driven by acute HFpEF. Survival at 1 year was poor regardless of EF but improved over time for black women and black men.
Keywords: ejection fraction; epidemiology; heart failure; mortality; race.
© 2018 American Heart Association, Inc.
Figures
Comment in
-
Heart Failure Epidemic: It's Complicated….Circulation. 2018 Jul 3;138(1):25-28. doi: 10.1161/CIRCULATIONAHA.118.028478. Circulation. 2018. PMID: 29967230 No abstract available.
References
-
- Sidney S, Rosamond WD, Howard VJ, Luepker RV, National Forum for Heart D. Stroke P. The “heart disease and stroke statistics–2013 update” and the need for a national cardiovascular surveillance system. Circulation. 2013;127:21–23. - PubMed
-
- Institute of Medicine (US) Committee on a National Surveillance System for Cardiovascular and Select Chronic Diseases. A Nationwide Framework for Surveillance of Cardiovascular and Chronic Lung Diseases. Washington DC: National Academies Press; 2011. - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, Cushman M, Das SR, de Ferranti S, Despres JP, Fullerton HJ, Howard VJ, Huffman MD, Isasi CR, Jimenez MC, Judd SE, Kissela BM, Lichtman JH, Lisabeth LD, Liu S, Mackey RH, Magid DJ, McGuire DK, Mohler ER, 3rd, Moy CS, Muntner P, Mussolino ME, Nasir K, Neumar RW, Nichol G, Palaniappan L, Pandey DK, Reeves MJ, Rodriguez CJ, Rosamond W, Sorlie PD, Stein J, Towfighi A, Turan TN, Virani SS, Woo D, Yeh RW, Turner MB, American Heart Association Statistics C and Stroke Statistics S Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133:e38–e360. - PubMed
-
- Heidenreich PA, Albert NM, Allen LA, Bluemke DA, Butler J, Fonarow GC, Ikonomidis JS, Khavjou O, Konstam MA, Maddox TM, Nichol G, Pham M, Pina IL, Trogdon JG, American Heart Association Advocacy Coordinating C, Council on Arteriosclerosis T, Vascular B, Council on Cardiovascular R, Intervention, Council on Clinical C, Council on E Prevention. Stroke C. Forecasting the impact of heart failure in the United States: a policy statement from the American Heart Association. Circ Heart Fail. 2013;6:606–619. - PMC - PubMed
Publication types
MeSH terms
Grants and funding
- HHSN268201100012C/HL/NHLBI NIH HHS/United States
- HHSN268201100009I/HL/NHLBI NIH HHS/United States
- HHSN268201100010C/HL/NHLBI NIH HHS/United States
- HHSN268201100008C/HL/NHLBI NIH HHS/United States
- HHSN268201100005G/HL/NHLBI NIH HHS/United States
- HHSN268201100008I/HL/NHLBI NIH HHS/United States
- HHSN268201100007C/HL/NHLBI NIH HHS/United States
- HHSN268201100011I/HL/NHLBI NIH HHS/United States
- HHSN268201100011C/HL/NHLBI NIH HHS/United States
- HHSN268201100006C/HL/NHLBI NIH HHS/United States
- HHSN268201100005I/HL/NHLBI NIH HHS/United States
- HHSN268201100009C/HL/NHLBI NIH HHS/United States
- HHSN268201100005C/HL/NHLBI NIH HHS/United States
- HHSN268201100007I/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
