

Rates of change in FEV1 and DLCO as potential indicators for mTOR inhibitor therapy in premenopausal lymphangioleiomyomatosis patients
- PMID: 29519926
- PMCID: PMC8697860
- DOI: 10.1183/13993003.02258-2017
Rates of change in FEV1 and DLCO as potential indicators for mTOR inhibitor therapy in premenopausal lymphangioleiomyomatosis patients
Abstract
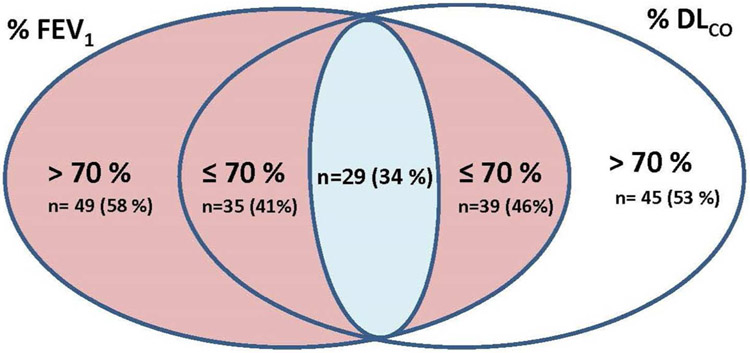
The value of rates of change in forced expiratory volume in 1 s (FEV1) and diffusing capacity of the lung for carbon monoxide (DLCO) to predict disease progression, and initiation of mTOR (mechanistic target of rapamycin) inhibitor therapy has not been evaluated.In 84 premenopausal lymphangioleiomyomatosis patients, individual rates of change in FEV1 and DLCO and their 95% confidence intervals were used to derive subsequent lowest values of FEV1 and DLCO that would prompt initiation of sirolimus therapy. These treatment criteria were compared with a criterion based on FEV1 or DLCO ≤70% predicted. In 12 patients undergoing sirolimus therapy both methods for determining the optimal point for initiation of therapy were evaluated.27 and 35 patients who experienced greater than expected rates of change in FEV1 and DLCO, respectively, would have been excluded from therapy based on an FEV1 or DLCO >70% pred. 25 of the 84 patients were eventually treated, but only when FEV1 or DLCO were ≤70% pred. Applying such treatment criteria to 12 patients undergoing sirolimus therapy would have delayed treatment for many years.Premenopausal females in whom FEV1 or DLCO are declining at rates above the expected based on their individual rates of decline, should be considered for sirolimus therapy before the FEV1 or DLCO falls to ≤70% pred.
The content of this work is not subject to copyright. Design and branding are copyright ©ERS 2018.
Conflict of interest statement
Conflict of interest: None declared.
Figures
Similar articles
-
Long-Term Effect of Sirolimus on Serum Vascular Endothelial Growth Factor D Levels in Patients With Lymphangioleiomyomatosis.Chest. 2018 Jan;153(1):124-132. doi: 10.1016/j.chest.2017.05.012. Epub 2017 May 19. Chest. 2018. PMID: 28533049 Free PMC article.
-
Changes in lung function and chylous effusions in patients with lymphangioleiomyomatosis treated with sirolimus.Ann Intern Med. 2011 Jun 21;154(12):797-805, W-292-3. doi: 10.7326/0003-4819-154-12-201106210-00007. Ann Intern Med. 2011. PMID: 21690594 Free PMC article.
-
Efficacy and safety of low-dose Sirolimus in Lymphangioleiomyomatosis.Orphanet J Rare Dis. 2018 Nov 14;13(1):204. doi: 10.1186/s13023-018-0946-8. Orphanet J Rare Dis. 2018. PMID: 30428897 Free PMC article.
-
Evolution of Diffusing Capacity of the Lungs for Carbon Monoxide in Lymphangioleiomyomatosis: Historical Perspectives and the Role of Advanced Imaging.Chest. 2025 Jun;167(6):1705-1713. doi: 10.1016/j.chest.2024.11.014. Epub 2024 Nov 21. Chest. 2025. PMID: 39580110 Review.
-
The efficacy and adverse events of mTOR inhibitors in lymphangioleiomyomatosis: systematic review and meta-analysis.Orphanet J Rare Dis. 2018 Aug 14;13(1):134. doi: 10.1186/s13023-018-0874-7. Orphanet J Rare Dis. 2018. PMID: 30107845 Free PMC article.
Cited by
-
Clinical, tomographic and functional comparison of sporadic and tuberous sclerosis complex-associated forms of lymphangioleiomyomatosis: a retrospective cohort study.ERJ Open Res. 2024 Mar 4;10(2):00759-2023. doi: 10.1183/23120541.00759-2023. eCollection 2024 Mar. ERJ Open Res. 2024. PMID: 38444661 Free PMC article.
-
Brazilian Thoracic Association recommendations for the management of lymphangioleiomyomatosis.J Bras Pneumol. 2025 Feb 10;51(1):e20240378. doi: 10.36416/1806-3756/e20240378. eCollection 2025. J Bras Pneumol. 2025. PMID: 39936727 Free PMC article. Review.
-
Pregnancy in lymphangioleiomyomatosis: clinical and lung function outcomes in two national cohorts.Thorax. 2020 Oct;75(10):904-907. doi: 10.1136/thoraxjnl-2020-214987. Epub 2020 Aug 11. Thorax. 2020. PMID: 32788260 Free PMC article.
-
Computer grading of lung disease severity in patients with lymphangioleiomyomatosis referred for transplantation.BMC Pulm Med. 2022 Sep 24;22(1):362. doi: 10.1186/s12890-022-02123-7. BMC Pulm Med. 2022. PMID: 36153516 Free PMC article.
-
Lymphangioleiomyomatosis and Pregnancy-Do We Have All the Answers for a Woman Who Desires to Conceive?-Literature Review.Cancers (Basel). 2025 Jan 20;17(2):323. doi: 10.3390/cancers17020323. Cancers (Basel). 2025. PMID: 39858105 Free PMC article. Review.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous