

Presentation of TRPM1-Associated Congenital Stationary Night Blindness in Children
- PMID: 29522070
- PMCID: PMC5876850
- DOI: 10.1001/jamaophthalmol.2018.0185
Presentation of TRPM1-Associated Congenital Stationary Night Blindness in Children
Abstract
Importance: Congenital stationary night blindness (CSNB) implies a stable condition, with the major symptom being nyctalopia present at birth. Pediatric clinical presentation and the course of different genetic subtypes of CSNB have not, to our knowledge, been well described in the era of molecular genetic diagnosis.
Objective: To describe the presentation and longitudinal clinical characteristics of pediatric patients with molecularly confirmed TRPM1-associated complete CSNB (cCSNB).
Design, setting, participants: This study was conducted at the University of Iowa from January 1, 1990, to July 1, 2015, and was a retrospective, longitudinal case series of 7 children (5 [71.4%] female) with TRPM1-associated cCSNB followed up for a mean (SD) of 11.1 (2.8) years.
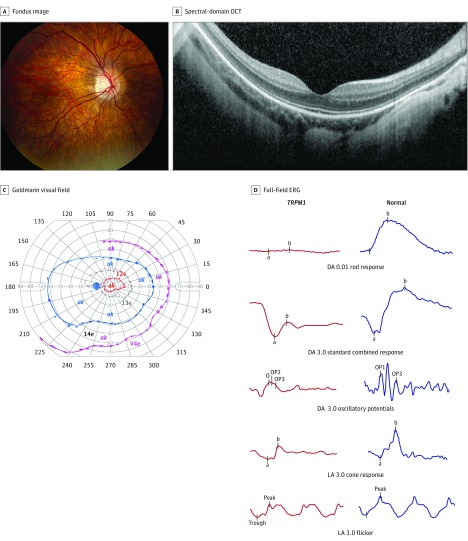
Main outcomes and measures: History, ophthalmologic examination findings, full-field electroretinogram (ffERG) results, full-field stimulus threshold testing results, Goldmann visual field results, optical coherence tomography results, and molecular genetic results were evaluated. Presenting symptoms and signs, the correlation of refractive error with electroretinography, and clinical evolution were analyzed.
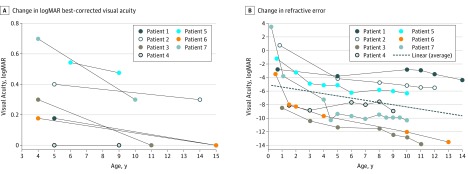
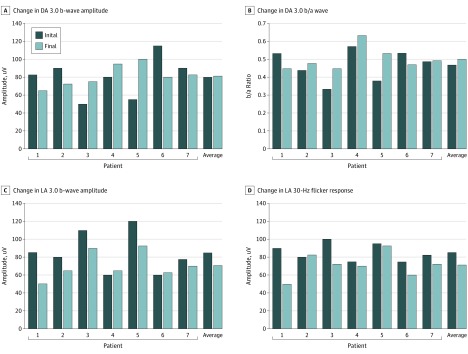
Results: Seven patients (5 [71.4%] female) presented early in childhood with strabismus (n = 6 [86%]), myopia (n = 5 [71%]), and/or nystagmus (n = 3 [43%]). The mean (SD) age at presentation was 8 (4) months and for receiving a diagnosis by ffERG was 7.3 years, with molecular diagnosis at 9.7 years. The mean (SD) length of follow-up was 11 (2.8) years. The best-corrected visual acuity at the most recent visit averaged 20/30 in the better-seeing eye (range, 20/20-20/60). The mean (SD) initial refraction was -2.80 (4.42) diopters (D) and the mean refraction at the most recent visit was -8.75 (3.53) D (range, -4.00 to -13.75 D), with the greatest rate of myopic shift before age 5 years. Full-field electroretinogram results were electronegative, consistent with cCSNB, without a significant change in amplitude over time. No patient or parent noted night blindness at presentation; however, subjective nyctalopia was eventually reported in 5 of 7 patients (71%). The full-field stimulus threshold testing results were moderately subnormal (-29.7 [3.8] dB; normal -59.8 [4.0] dB). Goldmann visual field results were significant for full I-4e, but constricted I-2e isopter. Eight different mutations or rare variants in TRPM1 predicted to be pathogenic were detected, with 3 novel variants.
Conclusions and relevance: Children with TRPM1-associated cCSNB presented before school age with progressive myopia as well as strabismus and nystagmus (but not nyctalopia), with stable, electronegative ffERG results, mildly subnormal full-field stimulus threshold testing results, and a constricted I2e isopter on perimetry. These findings suggest that ffERG and cCSNB genetic testing should be considered for children who present with early-onset myopia, especially in the presence of strabismus and/or nystagmus, and that TRPM1-associated cCSNB is a channelopathy that may present without complaints of night blindness in childhood.
Conflict of interest statement
Figures
Comment in
-
Revisiting Congenital Stationary Night Blindness in the Molecular Era.JAMA Ophthalmol. 2018 Apr 1;136(4):398-399. doi: 10.1001/jamaophthalmol.2018.0193. JAMA Ophthalmol. 2018. PMID: 29522064 No abstract available.
Similar articles
-
Congenital Stationary Night Blindness: Structure, Function and Genotype-Phenotype Correlations in a Cohort of 122 Patients.Ophthalmol Retina. 2024 Sep;8(9):932-941. doi: 10.1016/j.oret.2024.03.017. Epub 2024 Mar 24. Ophthalmol Retina. 2024. PMID: 38522615 Free PMC article.
-
Congenital Stationary Night Blindness due to Novel TRPM1 Gene Mutations in a Korean Patient.Korean J Ophthalmol. 2020 Apr;34(2):170-172. doi: 10.3341/kjo.2019.0080. Korean J Ophthalmol. 2020. PMID: 32233153 Free PMC article. No abstract available.
-
Congenital stationary night blindness with hypoplastic discs, negative electroretinogram and thinning of the inner nuclear layer.Graefes Arch Clin Exp Ophthalmol. 2016 Oct;254(10):1951-1956. doi: 10.1007/s00417-016-3346-6. Epub 2016 Apr 15. Graefes Arch Clin Exp Ophthalmol. 2016. PMID: 27084085
-
Congenital stationary night blindness: an update and review of the disease spectrum in Saudi Arabia.Acta Ophthalmol. 2021 Sep;99(6):581-591. doi: 10.1111/aos.14693. Epub 2020 Dec 26. Acta Ophthalmol. 2021. PMID: 33369259 Review.
-
[Overview of Congenital Stationary Night Blindness with Predominantly Normal Fundus Appearance].Klin Monbl Augenheilkd. 2018 Mar;235(3):281-289. doi: 10.1055/s-0043-123072. Epub 2018 Feb 1. Klin Monbl Augenheilkd. 2018. PMID: 29390235 Review. German.
Cited by
-
Improving the Yield of Genetic Diagnosis through Additional Genetic Panel Testing in Hereditary Ophthalmic Diseases.Curr Issues Mol Biol. 2024 May 20;46(5):5010-5022. doi: 10.3390/cimb46050300. Curr Issues Mol Biol. 2024. PMID: 38785568 Free PMC article.
-
Polyphenols and Visual Health: Potential Effects on Degenerative Retinal Diseases.Molecules. 2021 Jun 4;26(11):3407. doi: 10.3390/molecules26113407. Molecules. 2021. PMID: 34199888 Free PMC article. Review.
-
Full-field stimulus threshold testing: a scoping review of current practice.Eye (Lond). 2024 Jan;38(1):33-53. doi: 10.1038/s41433-023-02636-3. Epub 2023 Jul 13. Eye (Lond). 2024. PMID: 37443335 Free PMC article.
-
Clinical and genetic studies for a cohort of patients with congenital stationary night blindness.Orphanet J Rare Dis. 2024 Mar 6;19(1):101. doi: 10.1186/s13023-024-03091-3. Orphanet J Rare Dis. 2024. PMID: 38448886 Free PMC article.
-
Deep cross-modal feature learning applied to predict acutely decompensated heart failure using in-home collected electrocardiography and transthoracic bioimpedance.Artif Intell Med. 2023 Jun;140:102548. doi: 10.1016/j.artmed.2023.102548. Epub 2023 Apr 11. Artif Intell Med. 2023. PMID: 37210152 Free PMC article.
References
-
- Zeitz C, Robson AG, Audo I. Congenital stationary night blindness: an analysis and update of genotype-phenotype correlations and pathogenic mechanisms. Prog Retin Eye Res. 2015;45:58-110. - PubMed
-
- Bech-Hansen NT, Naylor MJ, Maybaum TA, et al. . Mutations in NYX, encoding the leucine-rich proteoglycan nyctalopin, cause X-linked complete congenital stationary night blindness. Nat Genet. 2000;26(3):319-323. - PubMed
-
- Pusch CM, Zeitz C, Brandau O, et al. . The complete form of X-linked congenital stationary night blindness is caused by mutations in a gene encoding a leucine-rich repeat protein. Nat Genet. 2000;26(3):324-327. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
