

Association of Survival With Shorter Time to Radiation Therapy After Surgery for US Patients With Head and Neck Cancer
- PMID: 29522072
- PMCID: PMC5876822
- DOI: 10.1001/jamaoto.2017.3406
Association of Survival With Shorter Time to Radiation Therapy After Surgery for US Patients With Head and Neck Cancer
Abstract
Importance: Shortening the time from surgery to the start of radiation (TS-RT) is a consideration for physicians and patients. Although the National Comprehensive Cancer Network recommends radiation to start within 6 weeks, a survival benefit with this metric remains controversial.
Objective: To determine the association of delayed TS-RT with overall survival (OS) using a large cancer registry.
Design, setting, and participants: In this observational cohort study, 25 216 patients with nonmetastatic stages III to IV head and neck cancer were identified from the National Cancer Database (NCDB).
Exposures: Patients received definitive surgery followed by adjuvant radiation therapy, with an interval duration defined as TS-RT.
Main outcomes and measures: Overall survival as a function of TS-RT and the effect of clinicopathologic risk factors and accelerated fractionation.
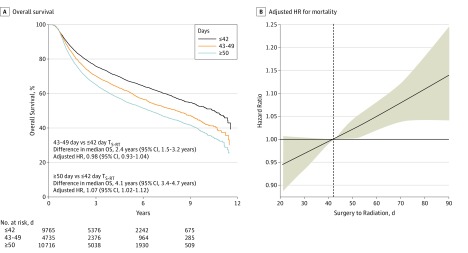
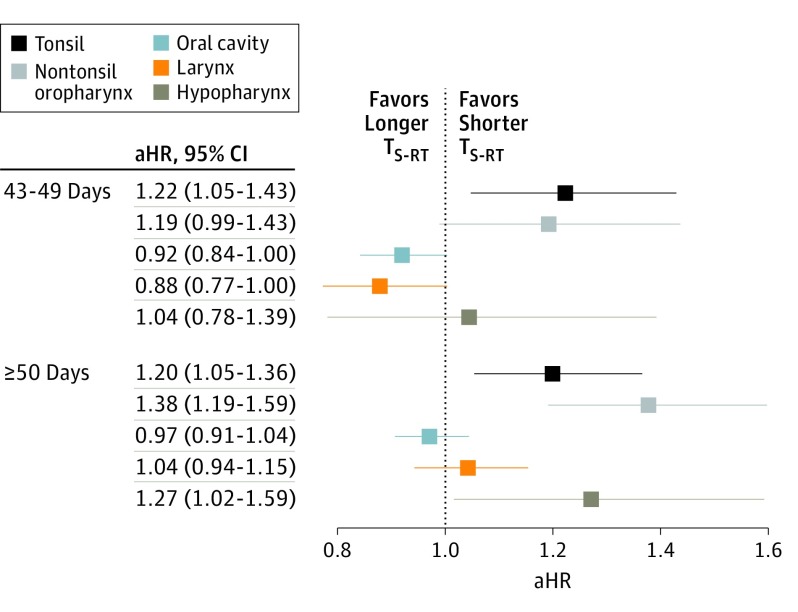
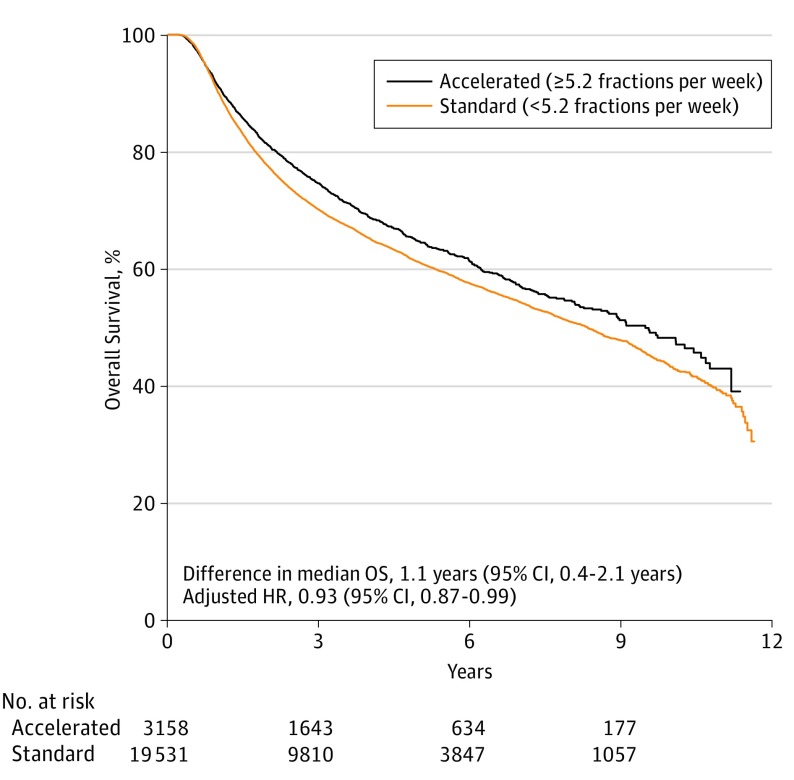
Results: We identified 25 216 patients with nonmetastatic squamous cell carcinoma of the head and neck. There were 18 968 (75%) men and 6248 (25%) women and the mean (SD) age of the cohort was 59 (10.9) years. Of the 25 216 patients, 9765 (39%) had a 42-days or less TS-RT and 4735 (19%) had a 43- to 49-day TS-RT. Median OS was 10.5 years (95% CI, 10.0-11.1 years) for patients with a 42-days or less TS-RT, 8.2 years (95% CI, 7.4-8.6 years; absolute difference, -2.4 years, 95% CI, -1.5 to -3.2 years) for patients with a 43- to 49-day TS-RT, and 6.5 years (95% CI, 6.1-6.8 years; absolute difference, -4.1 years, 95% CI, -3.4 to -4.7 years) for those with a 50-days or more TS-RT. Multivariable analysis found that compared with a 42-days or less TS-RT, there was not a significant increase in mortality with a 43- to 49-day TS-RT (HR, 0.98; 95% CI, 0.93-1.04), although there was for a TS-RT of 50 days or more (HR, 1.07; 95% CI, 1.02-1.12). A significant interaction was identified between TS-RT and disease site. Subgroup effect modeling found that a delayed TS-RT of 7 days resulted in significantly worse OS for patients with tonsil tumors (HR, 1.22; 95% CI, 1.05-1.43) though not other tumor subtypes. Accelerated fractionation of 5.2 fractions or more per week was associated with improved survival (HR, 0.93; 95% CI, 0.87-0.99) compared with standard fractionation.
Conclusions and relevance: Delayed TS-RT of 50 days or more was associated with worse overall survival. The multidisciplinary care team should focus on shortening TS-RT to improve survival. Unavoidable delays may be an indication for accelerated fractionation or other dose intensification strategies.
Conflict of interest statement
Figures
References
-
- Kramer S, Gelber RD, Snow JB, et al. Combined radiation therapy and surgery in the management of advanced head and neck cancer: final report of study 73-03 of the Radiation Therapy Oncology Group. Head Neck Surg. 1987;10(1):19-30. - PubMed
-
- Peters LJ, Goepfert H, Ang KK, et al. Evaluation of the dose for postoperative radiation therapy of head and neck cancer: first report of a prospective randomized trial. Int J Radiat Oncol Biol Phys. 1993;26(1):3-11. - PubMed
-
- Frank JL, Garb JL, Kay S, et al. Postoperative radiotherapy improves survival in squamous cell carcinoma of the hypopharynx. Am J Surg. 1994;168(5):476-480. - PubMed
-
- Trotti A, Klotch D, Endicott J, Ridley M, Cantor A. Postoperative accelerated radiotherapy in high-risk squamous cell carcinoma of the head and neck: long-term results of a prospective trial. Head Neck. 1998;20(2):119-123. - PubMed
-
- Lundahl RE, Foote RL, Bonner JA, et al. Combined neck dissection and postoperative radiation therapy in the management of the high-risk neck: a matched-pair analysis. Int J Radiat Oncol Biol Phys. 1998;40(3):529-534. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
