

A Controlled Trial of Mass Drug Administration to Interrupt Transmission of Multidrug-Resistant Falciparum Malaria in Cambodian Villages
- PMID: 29522113
- PMCID: PMC6117448
- DOI: 10.1093/cid/ciy196
A Controlled Trial of Mass Drug Administration to Interrupt Transmission of Multidrug-Resistant Falciparum Malaria in Cambodian Villages
Abstract
Background: The increase in multidrug-resistant Plasmodium falciparum in Southeast Asia suggests a need for acceleration of malaria elimination. We evaluated the effectiveness and safety of mass drug administration (MDA) to interrupt malaria transmission.
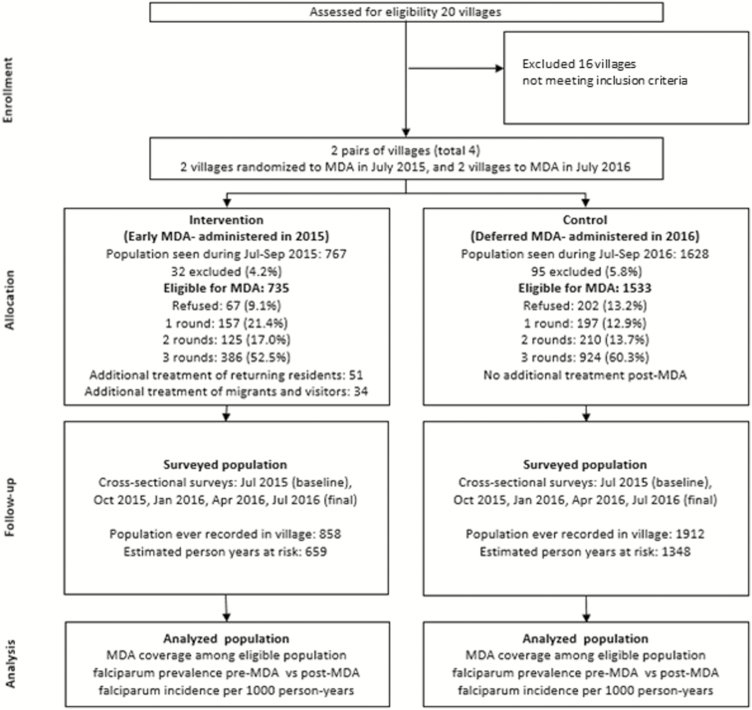
Methods: Four malaria-endemic villages in western Cambodia were randomized to 3 rounds of MDA (a 3-day course of dihydroartemisinin with piperaquine-phosphate), administered either early in or at the end of the study period. Comprehensive malaria treatment records were collected during 2014-2017. Subclinical parasite prevalence was estimated by ultrasensitive quantitative polymerase chain reaction quarterly over 12 months.
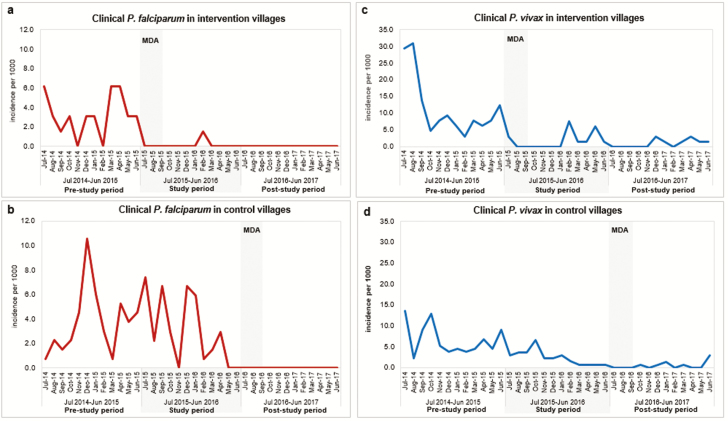
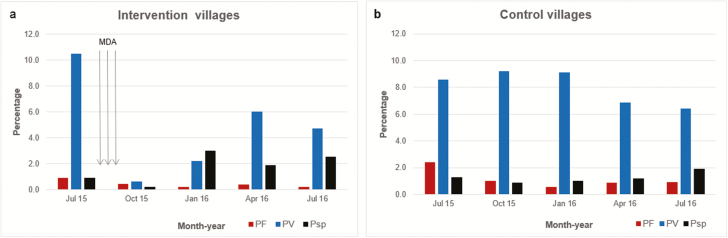
Results: MDA coverage with at least 1 complete round was 88% (1999/2268), ≥2 rounds 73% (1645/2268), and all 3 rounds 58% (1310/2268). Plasmodium falciparum incidence in intervention and control villages was similar over the 12 months prior to the study: 39 per 1000 person-years (PY) vs 45 per 1000 PY (P = .50). The primary outcome, P. falciparum incidence in the 12 months after MDA, was lower in intervention villages (1.5/1000 PY vs 37.1/1000 PY; incidence rate ratio, 24.5 [95% confidence interval], 3.4-177; P = .002). Following MDA in 2016, there were no clinical falciparum malaria cases over 12 months (0/2044 PY) in all 4 villages. Plasmodium vivax prevalence decreased markedly in intervention villages following MDA but returned to approximately half the baseline prevalence by 12 months. No severe adverse events were attributed to treatment.
Conclusions: Mass drug administrations achieved high coverage, were safe, and associated with the absence of clinical P. falciparum cases for at least 1 year.
Clinical trials registration: NCT01872702.
Figures

References
-
- Noedl H, Se Y, Schaecher K, Smith BL, Socheat D, Fukuda MM; Artemisinin Resistance in Cambodia 1 (ARC1) Study Consortium Evidence of artemisinin-resistant malaria in western Cambodia. N Engl J Med 2008; 359:2619–20. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
