

doi: 10.1093/eurheartj/ehy060.
Chronic kidney disease and arrhythmias: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference
Collaborators,
Affiliations
- PMID: 29522134
- PMCID: PMC6012907
- DOI: 10.1093/eurheartj/ehy060
Item in Clipboard
Chronic kidney disease and arrhythmias: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference
Eur Heart J.
.
No abstract available
Figures
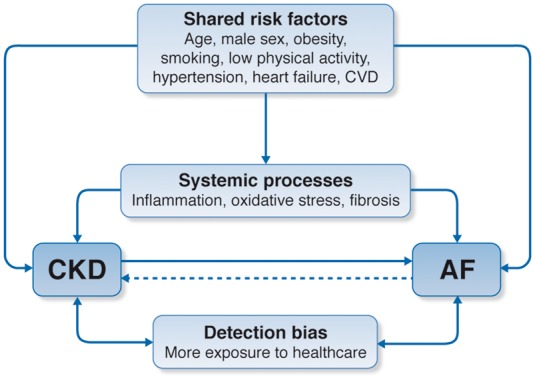
Relationship between chronic kidney disease and atrial fibrillation: shared risk factors and outcomes. Chronic kidney disease and atrial fibrillation share a number of risk factors and conditions that promote their incidence, possibly via systemic processes such as inflammation, oxidative stress, or fibrosis. It is established that chronic kidney disease increases the incidence of atrial fibrillation and there is some evidence to suggest that atrial fibrillation also increases chronic kidney disease progression. When examining the strength of these associations, we acknowledge the potential impact of detection bias in observational studies where more frequent exposure to healthcare likely prompts more clinical findings in this comorbid population. AF, atrial fibrillation; CKD, chronic kidney disease; CVD, cardiovascular disease.
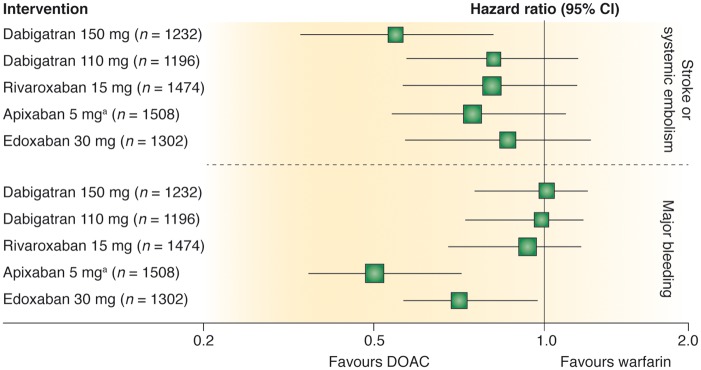
Efficacy and safety of direct oral anticoagulants (DOACs) vs. warfarin in the subgroup of patients with moderate chronic kidney disease from randomized controlled trials in atrial fibrillation. Comparison of hazard ratios and 95% confidence intervals for primary efficacy and safety outcomes for 150 and 110 mg dabigatran twice daily, 15 mg rivaroxaban once daily, 5 mg apixaban twice daily, and 30 mg edoxaban once daily. Chronic kidney disease was defined as estimated creatinine clearance of 30 to 49 mL/min or as 25 to 49 mL/min for apixaban. aApixaban 2.5 mg twice daily if patient had any two of the following: age ≥ 80 years, body weight ≤ 60 kg, or serum creatinine ≥1.5 mg/dL. Reproduced from Qamar and Bhatt with permission from the publisher.
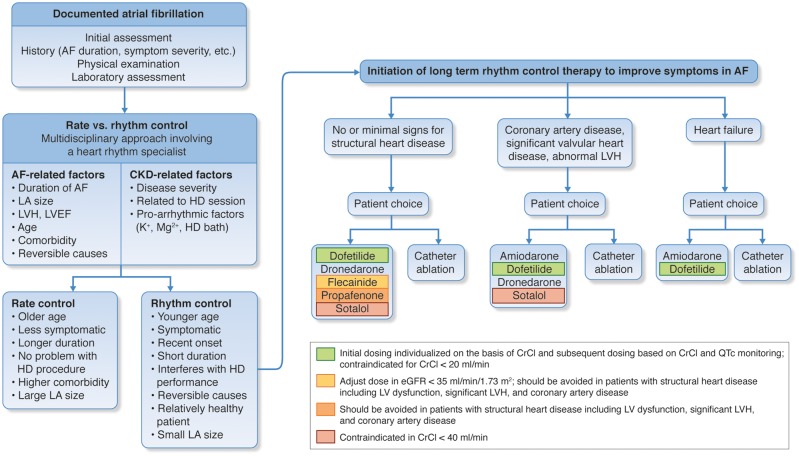
Algorithm for decision-making about rate vs. rhythm control in chronic kidney disease. Especially since chronic kidney disease patients show a lot of specific characteristics regarding history, comorbidities and personal preferences, in each patient an individualized decision should be made. Many aspects should be taken into account: the duration of atrial fibrillation, the symptom severity, renal clearance (risk of toxicity, dialyzability), and potential contraindications for antiarrhythmic drugs due to structural heart disease, which is very frequent in these patients (such as left ventricular hypertrophy, reduced ejection fraction, obstructive coronary artery disease). Moreover, proarrhythmic effects (such as QT prolongation) may be pronounced because of electrolyte imbalances in chronic kidney disease. The figure suggests an algorithm presenting the most relevant criteria that should be incorporated into a multidisciplinary decision-making process, including the treating nephrologist, a heart rhythm specialist, and eventually also physicians of other disciplines. Of note, regardless of which strategy is chosen, oral anticoagulation should always be administered in early stages of chronic kidney disease and at least be considered in advanced stages of chronic kidney disease (see section on Stroke prevention and oral anticoagulation). AF, atrial fibrillation; CKD, chronic kidney disease; EF, ejection fraction; eGFR, estimated glomerular filtration rate; HD, haemodialysis; LA, left atrial; LVEF, left ventricular ejection fraction; LVH, left ventricular hypertrophy. Adapted in part from Kirchhof et al.
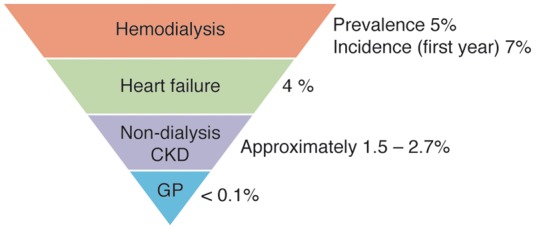
Annual rates of sudden cardiac death. CKD, chronic kidney disease; GP, general population.
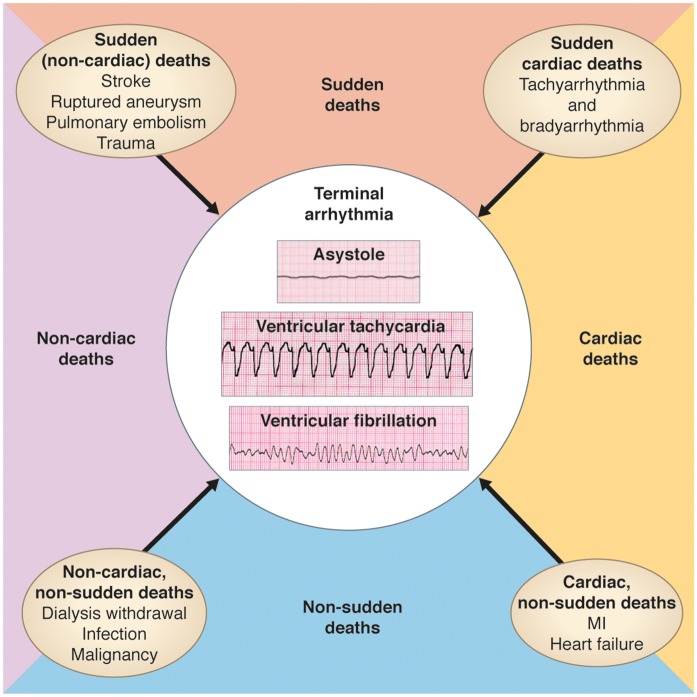
Mechanisms of death in chronic kidney disease patients.
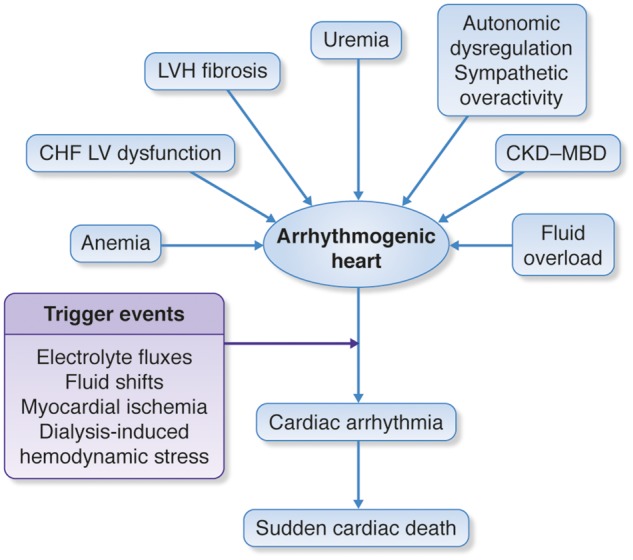
Potential predisposing factors of sudden cardiac death. CHF, congestive heart failure; CKD-MBD, chronic kidney disease-mineral and bone disorders; LV, left ventricular; LVH, left ventricular hypertrophy.
Comment in
-
Chronic kidney disease and arrhythmias: highlights from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference.Kidney Int. 2018 Aug;94(2):231-234. doi: 10.1016/j.kint.2018.05.005. Epub 2018 Jun 21. Kidney Int. 2018. PMID: 29935952 No abstract available.
References
-
- Konstantinidis I, Nadkarni GN, Yacoub R, Saha A, Simoes P, Parikh CR, Coca SG.. Representation of patients with kidney disease in trials of cardiovascular interventions: an updated systematic review. JAMA Intern Med 2016;176:121–124. - PubMed
-
- Boriani G, Savelieva I, Dan GA, Deharo JC, Ferro C, Israel CW, Lane DA, La Manna G, Morton J, Mitjans AM, Vos MA, Turakhia MP, Lip GY.. Chronic kidney disease in patients with cardiac rhythm disturbances or implantable electrical devices: clinical significance and implications for decision making-a position paper of the European Heart Rhythm Association endorsed by the Heart Rhythm Society and the Asia Pacific Heart Rhythm Society. Europace 2015;17:1169–1196. - PMC - PubMed
-
- Heidbuchel H, Verhamme P, Alings M, Antz M, Diener HC, Hacke W, Oldgren J, Sinnaeve P, Camm AJ, Kirchhof P.. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Europace 2015;17:1467–1507. - PubMed
-
- Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, Castella M, Diener HC, Heidbuchel H, Hendriks J, Hindricks G, Manolis AS, Oldgren J, Popescu BA, Schotten U, Van Putte B, Vardas P, Agewall S, Camm J, Baron Esquivias G, Budts W, Carerj S, Casselman F, Coca A, De Caterina R, Deftereos S, Dobrev D, Ferro JM, Filippatos G, Fitzsimons D, Gorenek B, Guenoun M, Hohnloser SH, Kolh P, Lip GY, Manolis A, McMurray J, Ponikowski P, Rosenhek R, Ruschitzka F, Savelieva I, Sharma S, Suwalski P, Tamargo JL, Taylor CJ, Van Gelder IC, Voors AA, Windecker S, Zamorano JL, Zeppenfeld K.. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016;37:2893–2962. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
