

Obesity as disruptor of the female fertility
- PMID: 29523133
- PMCID: PMC5845358
- DOI: 10.1186/s12958-018-0336-z
Obesity as disruptor of the female fertility
Abstract
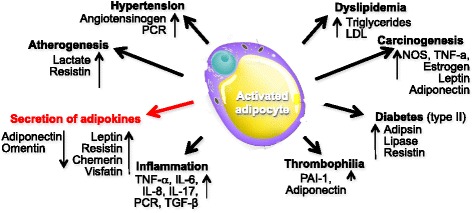
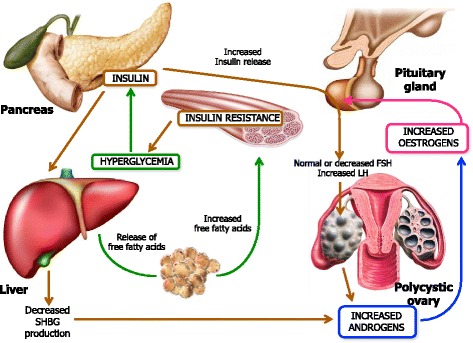
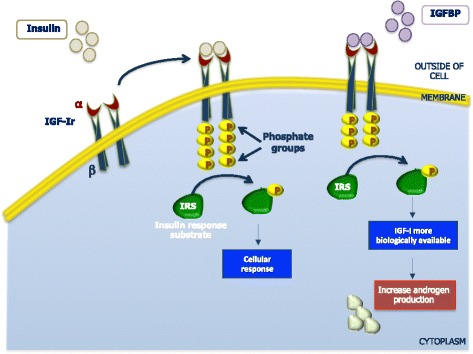
Both obesity and overweight are increasing worldwide and have detrimental influences on several human body functions including the reproductive health. In particular, obese women undergo perturbations of the 'hypothalamic pituitary ovarian axis', and frequently suffer of menstrual dysfunction leading to anovulation and infertility. Besides the hormone disorders and subfertility that are common in the polycystic ovary syndrome (PCOS), in obesity the adipocytes act as endocrine organ. The adipose tissue indeed, releases a number of bioactive molecules, namely adipokines, that variably interact with multiple molecular pathways of insulin resistance, inflammation, hypertension, cardiovascular risk, coagulation, and oocyte differentiation and maturation. Moreover, endometrial implantation and other reproductive functions are affected in obese women with complications including delayed conceptions, increased miscarriage rate, reduced outcomes in assisted conception treatments.On the contrary, weight loss programs through lifestyle modification in obese women, have been proven to restore menstrual cyclicity and ovulation and improve the likelihood of conception.
Keywords: Adipokines; Anovulation; Infertility; Obesity; Oocytes.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- McGee EA, Hsueh AJ. Initial and cyclic recruitment of ovarian follicles. Endocr Rev. 2000;21:200–214. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
