

Incidence and risk factors of neonatal infections in a rural Bangladeshi population: a community-based prospective study
- PMID: 29523194
- PMCID: PMC5845215
- DOI: 10.1186/s41043-018-0136-2
Incidence and risk factors of neonatal infections in a rural Bangladeshi population: a community-based prospective study
Abstract
Background: Infections cause about one fifth of the estimated 2.7 million annual neonatal deaths worldwide. Population-based data on burden and risk factors of neonatal infections are lacking in developing countries, which are required for the appropriate design of effective preventive and therapeutic interventions in resource-poor settings.
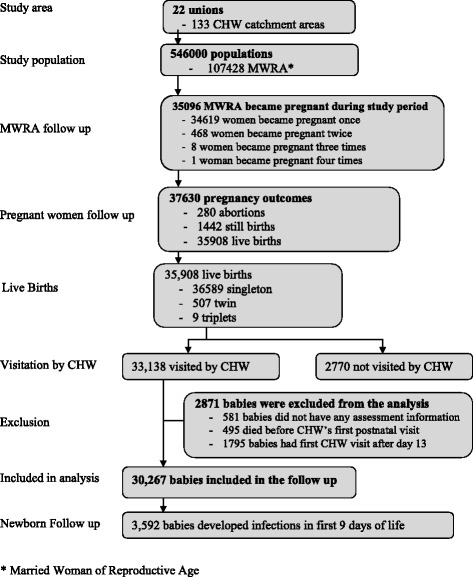
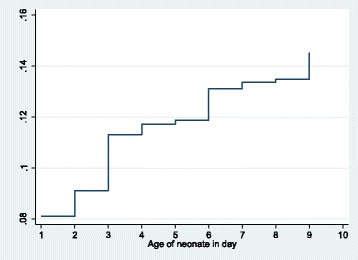
Methods: We used data from a community-based cluster-randomized trial conducted to evaluate the impact of two umbilical cord cleansing regimens with chlorhexidine solution on neonatal mortality and morbidity in a rural area of Sylhet District in Bangladesh. Newborns were assessed four times in the first 9 days of life by trained community health workers (CHWs) using a WHO IMCI-like clinical algorithm. Cumulative incidence of the first episode of infections in the first 9 days of life was estimated using survival analysis technique accounting for survival bias and competing risk of death before the occurrence of infection. A multivariable generalized estimating equation log-binomial regression model was used to identify factors independently associated with infections.
Results: Between 2007 and 2009, 30,267 newborns who received at least one postnatal assessment visit by a CHW within the first 9 days of life were included in this study. Cumulative incidence of infections in the first 9 days of life was 14.5% (95% CI 14.1-14.9%). Significant risk factors included previous child death in the family [RR 1.10 (95% CI 1.02-1.19)]; overcrowding [RR 1.14 (95% CI 1.04-1.25)]; home delivery [RR 1.86 (95% CI 1.58-2.19)]; unclean cord care [RR 1.15 (95% CI 1.03-1.28)]; multiple births [RR 1.34 (95% CI 1.15-1.56)]; low birth weight [reference: ≥ 2500 g, RR (95% CI) for < 1500, 1500-1999, and 2000-2499 g were 4.69 (4.01-5.48), 2.15 (1.92-2.42), and 1.15 (1.07-1.25) respectively]; and birth asphyxia [RR 1.65 (1.51-1.81)]. Higher pregnancy order lowered the risk of infections in the study population [compared to first pregnancy, RR (95% CI) for second, third, and ≥ fourth pregnancy babies were 0.93 (0.85-1.02), 0.88 (0.79-0.97), and 0.79 (0.71-0.87), respectively].
Conclusion: Neonatal infections and associated deaths can be reduced by identifying and following up high-risk mothers and newborns and promoting facility delivery and clean cord care in resource-poor countries like Bangladesh where the burden of clinically ascertained neonatal infections is high. Further research is needed to measure the burden of infections in the entire neonatal period, particularly in the second fortnight and its association with essential newborn care.
Trial registration: NCT00434408 . Registered February 9, 2007.
Keywords: Bangladesh; Neonatal infections; Prospective study; Risk factors.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was approved by the Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health and the Ethical Review Committee of the International Centre for Diarrheal Disease Research, Bangladesh (icddr,b). Oral consent was obtained from each respondent prior to the data collection. Privacy and confidentiality were maintained throughout the study.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
The effect of cord cleansing with chlorhexidine on neonatal mortality in rural Bangladesh: a community-based, cluster-randomised trial.Lancet. 2012 Mar 17;379(9820):1022-8. doi: 10.1016/S0140-6736(11)61848-5. Epub 2012 Feb 8. Lancet. 2012. PMID: 22322124 Clinical Trial.
-
Impact of 4.0% chlorhexidine cleansing of the umbilical cord on mortality and omphalitis among newborns of Sylhet, Bangladesh: design of a community-based cluster randomized trial.BMC Pediatr. 2009 Oct 21;9:67. doi: 10.1186/1471-2431-9-67. BMC Pediatr. 2009. PMID: 19845951 Free PMC article. Clinical Trial.
-
Neonatal mortality risks among preterm births in a rural Bangladeshi cohort.Paediatr Perinat Epidemiol. 2014 Nov;28(6):510-20. doi: 10.1111/ppe.12145. Epub 2014 Sep 16. Paediatr Perinat Epidemiol. 2014. PMID: 25223240 Clinical Trial.
-
Safety and impact of chlorhexidine antisepsis interventions for improving neonatal health in developing countries.Pediatr Infect Dis J. 2006 Aug;25(8):665-75. doi: 10.1097/01.inf.0000223489.02791.70. Pediatr Infect Dis J. 2006. PMID: 16874163 Free PMC article. Review.
-
Essential childbirth and postnatal interventions for improved maternal and neonatal health.Reprod Health. 2014;11 Suppl 1(Suppl 1):S3. doi: 10.1186/1742-4755-11-S1-S3. Epub 2014 Aug 21. Reprod Health. 2014. PMID: 25177795 Free PMC article. Review.
Cited by
-
Prevalence of common symptoms of neonatal illness in Northwest Ethiopia: A repeated measure cross-sectional study.PLoS One. 2021 Mar 30;16(3):e0248678. doi: 10.1371/journal.pone.0248678. eCollection 2021. PLoS One. 2021. PMID: 33784322 Free PMC article.
-
Bacteriological profile, antibiotic susceptibility and factors associated with neonatal Septicaemia at Kilembe mines hospital, Kasese District Western Uganda.BMC Microbiol. 2021 Nov 4;21(1):303. doi: 10.1186/s12866-021-02367-z. BMC Microbiol. 2021. PMID: 34736415 Free PMC article.
-
Prevalence and Associated Risk Factors of Sepsis among Neonates Admitted into Neonatal Intensive Care Units of Public Hospitals in Dhaka.Cureus. 2020 Mar 29;12(3):e7461. doi: 10.7759/cureus.7461. Cureus. 2020. PMID: 32351840 Free PMC article.
-
Association of low vitamin D level and full-term early-onset neonatal sepsis; a case-control study.Ital J Pediatr. 2024 May 18;50(1):101. doi: 10.1186/s13052-024-01665-2. Ital J Pediatr. 2024. PMID: 38762477 Free PMC article.
-
Community health workers and health equity in low- and middle-income countries: systematic review and recommendations for policy and practice.Int J Equity Health. 2022 Apr 11;21(1):49. doi: 10.1186/s12939-021-01615-y. Int J Equity Health. 2022. PMID: 35410258 Free PMC article.
References
-
- Liu L, Hill K, Oza S, Hogan D, Chu Y, Cousens S, Mathers C, Stanton C, Lawn J, Black RE. Levels and causes of mortality under age five years. In: Black RE, Laxminarayan R, Temmrman M, Walker N, editors. Reproductive, maternal, newborn, and child health. Volume 1. Third. Washington DC: World Bank Group; 2016. p. 74. - PubMed
-
- Oestergaard MZ, Inoue M, Yoshida S, Mahanani WR, Gore FM, Cousens S, Lawn JE, Mathers CD, United Nations Inter-Agency Group for Child Mortality E, the Child Health Epidemiology Reference G Neonatal mortality levels for 193 countries in 2009 with trends since 1990: a systematic analysis of progress, projections, and priorities. PLoS Med. 2011;8(8):e1001080. doi: 10.1371/journal.pmed.1001080. - DOI - PMC - PubMed
-
- UNICEF . Levels and trends in child mortality: report 2014. Estimates developed by the UN Inter-agency Group for Child Morality Estimation. New York: UNICEF; 2014.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
