

Long-term clinical parameters after switching to nocturnal haemodialysis: a Dutch propensity-score-matched cohort study comparing patients on nocturnal haemodialysis with patients on three-times-a-week haemodialysis/haemodiafiltration
- PMID: 29523566
- PMCID: PMC5855195
- DOI: 10.1136/bmjopen-2017-019900
Long-term clinical parameters after switching to nocturnal haemodialysis: a Dutch propensity-score-matched cohort study comparing patients on nocturnal haemodialysis with patients on three-times-a-week haemodialysis/haemodiafiltration
Abstract
Objectives: Nocturnal haemodialysis (NHD), characterised by 8-hour sessions ≥3 times a week, is known to improve clinical parameters in the short term compared with conventional-schedule haemodialysis (HD), generally 3×3.5-4 hours a week. We studied long-term effects of NHD and used patients on conventional HD/haemodiafiltration (HDF) as controls.
Design: Four-year prospective follow-up of patients who switched to NHD; we compared patients with patients on HD/HDF using propensity score matching.
Setting: 28 Dutch dialysis centres.
Participants: We included 159 patients starting with NHD any time since 2004, aged 56.7±12.9 years, with median dialysis vintage 2.3 (0.9-5.1) years. We propensity-score matched 100 patients on NHD to 100 on HD/HDF.
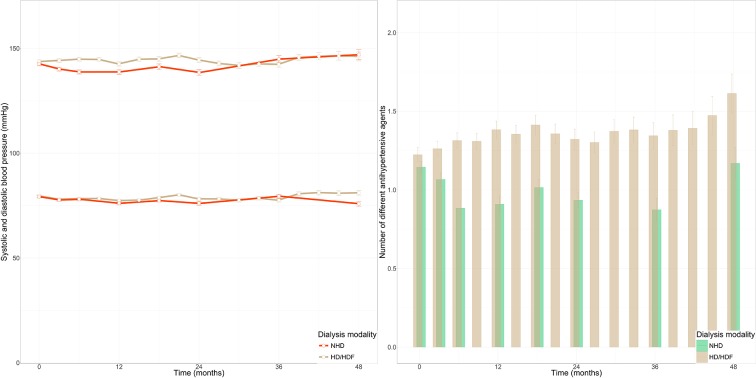
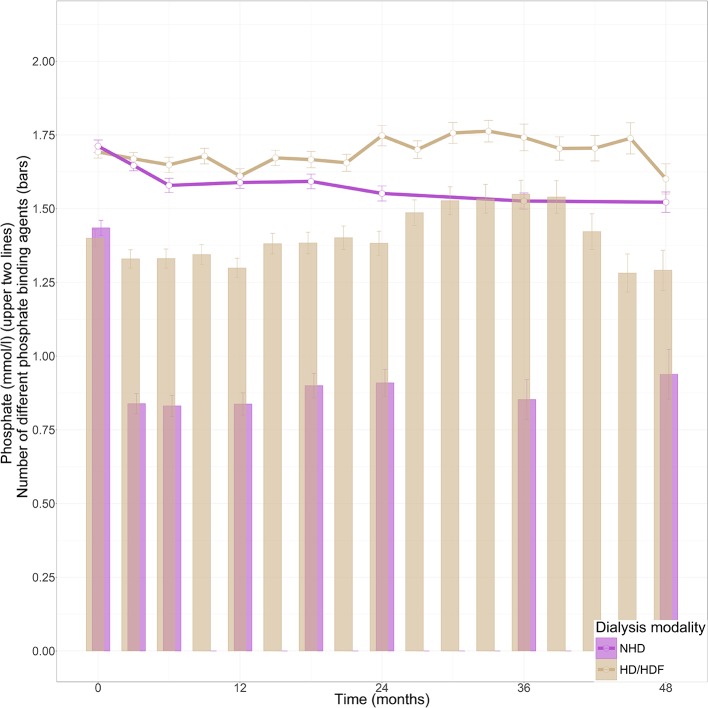
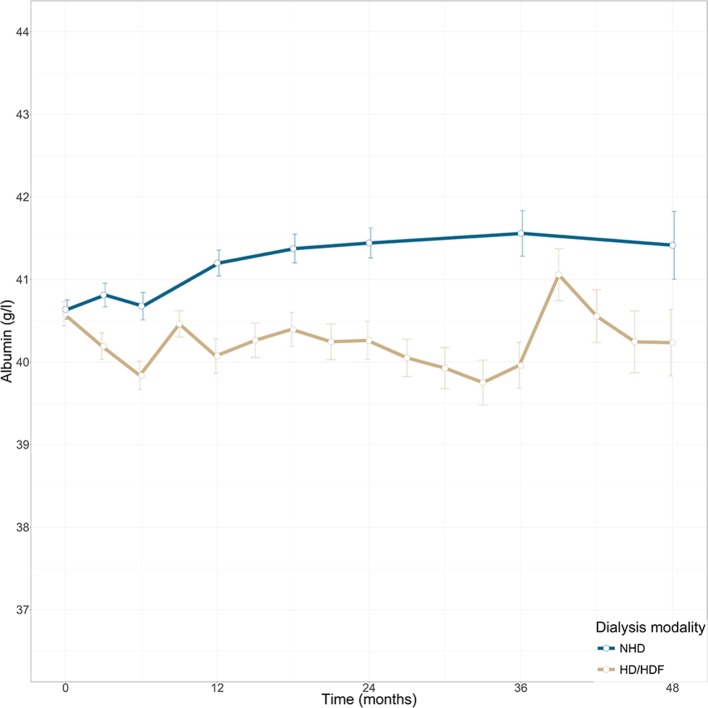
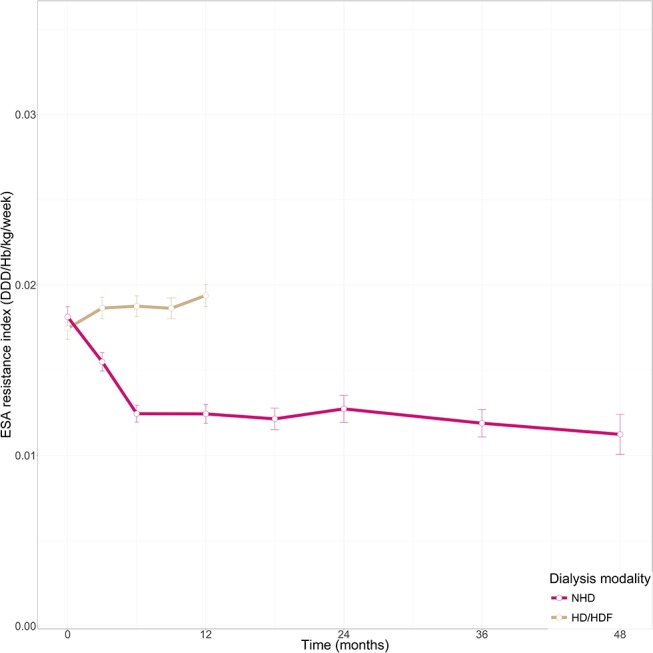
Primary and secondary outcome measures: Control of hypertension (predialysis blood pressure, number of antihypertensives), phosphate (phosphate, number of phosphate binders), nutritional status and inflammation (albumin, C reactive protein and postdialysis weight) and anaemia (erythropoiesis-stimulating agent (ESA) resistance).
Results: Switching to NHD was associated with a non-significant reduction of antihypertensives compared with HD/HDF (OR <2 types 2.17, 95% CI 0.86 to 5.50, P=0.11); and a prolonged lower need for phosphate binders (OR <2 types 1.83, 95% CI 1.10 to 3.03, P=0.02). NHD was not associated with significant changes in blood pressure or phosphate. NHD was associated with significantly higher albumin over time compared with HD/HDF (0.70 g/L/year, 95% CI 0.10 to 1.30, P=0.02). ESA resistance decreased significantly in NHD compared with HD/HDF, resulting in a 33% lower ESA dose in the long term.
Conclusions: After switching to NHD, the lower need for antihypertensives, phosphate binders and ESA persists for at least 4 years. These sustained improvements in NHD contrast significantly with the course of these parameters during continued treatment with conventional-schedule HD and HDF. NHD provides an optimal form of dialysis, also suitable for patients expected to have a long waiting time for transplantation or those convicted to indefinite dialysis.
Keywords: albumin; erythropoietin; haemodialysis; nocturnal haemodialysis; phosphate binders; propensity score matching.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: MPCG reports personal fees and non-financial support from Baxter Healthcare and personal fees from Fresenius Medical Care Netherlands, outside the submitted work.
Figures
Similar articles
-
Online-haemodiafiltration vs. conventional haemodialysis: a cross-over study.BMC Nephrol. 2015 May 9;16:70. doi: 10.1186/s12882-015-0062-0. BMC Nephrol. 2015. PMID: 25956949 Free PMC article.
-
High-volume online haemodiafiltration improves erythropoiesis-stimulating agent (ESA) resistance in comparison with low-flux bicarbonate dialysis: results of the REDERT study.Nephrol Dial Transplant. 2015 Apr;30(4):682-9. doi: 10.1093/ndt/gfu345. Epub 2014 Nov 10. Nephrol Dial Transplant. 2015. PMID: 25385719 Clinical Trial.
-
High-efficiency on-line haemodiafiltration improves conduit artery endothelial function compared with high-flux haemodialysis in end-stage renal disease patients.Nephrol Dial Transplant. 2014 Feb;29(2):414-22. doi: 10.1093/ndt/gft448. Epub 2013 Nov 13. Nephrol Dial Transplant. 2014. PMID: 24235073 Clinical Trial.
-
Current Evidence in Haemodiafiltration.Blood Purif. 2015;40 Suppl 1:24-9. doi: 10.1159/000437410. Epub 2015 Sep 8. Blood Purif. 2015. PMID: 26344510 Review.
-
Clinical evidence on haemodiafiltration.Nephrol Dial Transplant. 2018 Oct 1;33(suppl_3):iii53-iii58. doi: 10.1093/ndt/gfy218. Nephrol Dial Transplant. 2018. PMID: 30281128 Free PMC article. Review.
Cited by
-
Nocturnal Hemodialysis Leads to Improvement in Physical Performance in Comparison with Conventional Hemodialysis.Nutrients. 2022 Dec 29;15(1):168. doi: 10.3390/nu15010168. Nutrients. 2022. PMID: 36615825 Free PMC article.
-
Physical performance in patients treated with nocturnal hemodialysis - a systematic review of the evidence.BMC Nephrol. 2019 Aug 14;20(1):317. doi: 10.1186/s12882-019-1518-4. BMC Nephrol. 2019. PMID: 31412793 Free PMC article.
-
Health-related quality of life compared between kidney transplantation and nocturnal hemodialysis.PLoS One. 2018 Sep 20;13(9):e0204405. doi: 10.1371/journal.pone.0204405. eCollection 2018. PLoS One. 2018. PMID: 30235331 Free PMC article.
-
Anemia management for home dialysis including the new US public policy initiative.Kidney Int Suppl (2011). 2021 Apr;11(1):59-69. doi: 10.1016/j.kisu.2020.12.005. Epub 2021 Mar 18. Kidney Int Suppl (2011). 2021. PMID: 33777496 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials