

Cognitive-behavioural therapy (CBT) for renal fatigue (BReF): a feasibility randomised-controlled trial of CBT for the management of fatigue in haemodialysis (HD) patients
- PMID: 29523571
- PMCID: PMC5855165
- DOI: 10.1136/bmjopen-2017-020842
Cognitive-behavioural therapy (CBT) for renal fatigue (BReF): a feasibility randomised-controlled trial of CBT for the management of fatigue in haemodialysis (HD) patients
Abstract
Introduction: Fatigue is one of the most common and disabling symptoms in end-stage kidney disease, particularly among in-centre haemodialysis patients. This two-arm parallel group feasibility randomised controlled trial will determine whether a fully powered efficacy trial is achievable by examining the feasibility of recruitment, acceptability and potential benefits of a cognitive-behavioural therapy (CBT)-based intervention for fatigue among in-centre haemodialysis patients.
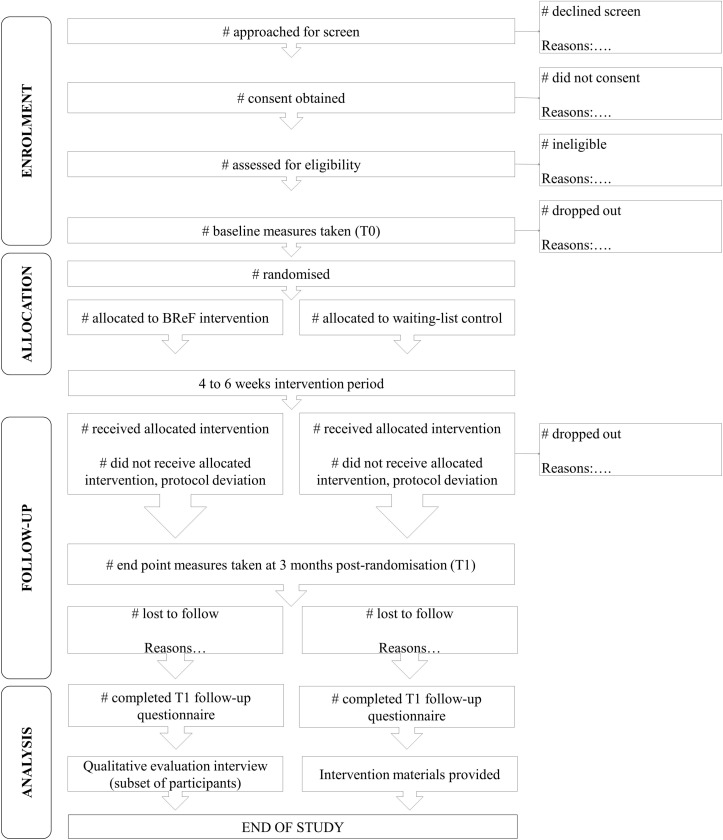
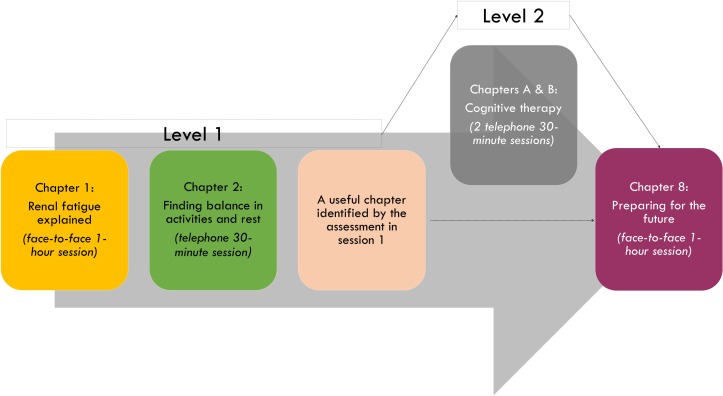
Methods: We aim to recruit 40 adult patients undergoing in-centre haemodialysis at secondary care outpatient dialysis units, who meet clinical levels of fatigue. Patients will be randomised individually (using a 1:1 ratio) to either a 4-6 weeks' CBT-based intervention (intervention arm) or to a waiting-list control (control arm). The primary feasibility outcomes include descriptive data on numbers within each recruiting centre meeting eligibility criteria, rates of recruitment, numbers retained postrandomisation and treatment adherence. To assess the potential benefits of the cognitive-behavioural therapy for renal fatigue intervention, secondary self-report outcomes include measures of fatigue severity (Chalder Fatigue Questionnaire), fatigue-related functional impairment (Work and Social Adjustment Scale), sleep quality (Pittsburgh Sleep Quality Index), depression (Patient Health Questionnaire-9) and anxiety (Generalised Anxiety Disorder-7). Changes in fatigue perceptions (Brief Illness Perception Questionnaire), cognitive and behavioural responses to fatigue (Cognitive and Behavioural Responses to Symptoms Questionnaire), sleep hygiene behaviours (Sleep Hygiene Index) and physical activity (International Physical Activity Questionnaire-short form) will also be explored. These self-report measures will be collected at baseline and 3 months postrandomisation. Nested qualitative interviews will be conducted postintervention to explore the acceptability of the intervention and identify any areas in need of improvement. The statistician and assessor will be blinded to treatment allocation.
Ethics and dissemination: A National Health Service (NHS) Research Ethics Committee approved the study. Any amendments to the protocol will be submitted to the NHS Committee and study sponsor.
Trial registration number: ISRCTN91238019;Pre-results.
Keywords: cognitive behavioural therapy; dialysis; fatigue; kidney failure; quality of life.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical