

Assessment of temporally-related acute respiratory illness following influenza vaccination
- PMID: 29525279
- PMCID: PMC7115556
- DOI: 10.1016/j.vaccine.2018.02.105
Assessment of temporally-related acute respiratory illness following influenza vaccination
Abstract
Background: A barrier to influenza vaccination is the misperception that the inactivated vaccine can cause influenza. Previous studies have investigated the risk of acute respiratory illness (ARI) after influenza vaccination with conflicting results. We assessed whether there is an increased rate of laboratory-confirmed ARI in post-influenza vaccination periods.
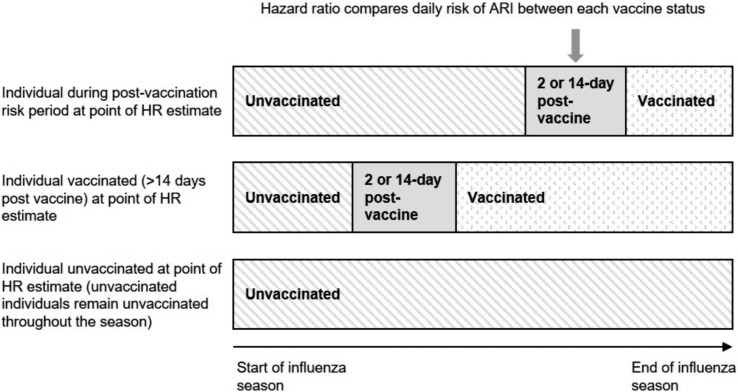
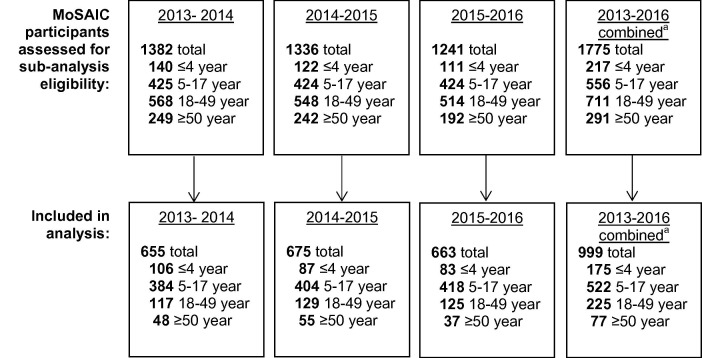
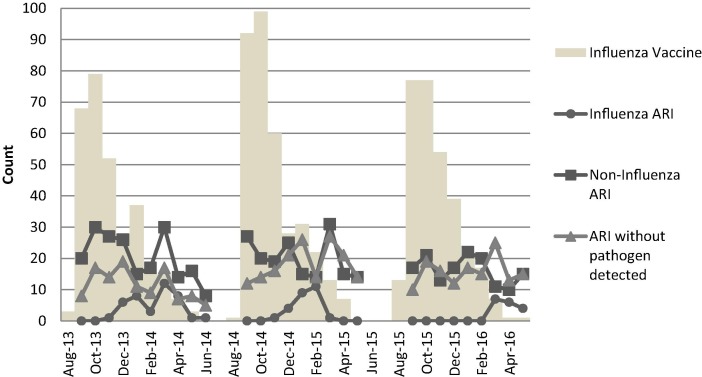
Methods: We conducted a cohort sub-analysis of children and adults in the MoSAIC community surveillance study from 2013 to 2016. Influenza vaccination was confirmed through city or hospital registries. Cases of ARI were ascertained by twice-weekly text messages to household to identify members with ARI symptoms. Nasal swabs were obtained from ill participants and analyzed for respiratory pathogens using multiplex PCR. The primary outcome measure was the hazard ratio of laboratory-confirmed ARI in individuals post-vaccination compared to other time periods during three influenza seasons.
Results: Of the 999 participants, 68.8% were children, 30.2% were adults. Each study season, approximately half received influenza vaccine and one third experienced ≥1 ARI. The hazard of influenza in individuals during the 14-day post-vaccination period was similar to unvaccinated individuals during the same period (HR 0.96, 95% CI [0.60, 1.52]). The hazard of non-influenza respiratory pathogens was higher during the same period (HR 1.65, 95% CI [1.14, 2.38]); when stratified by age the hazard remained higher for children (HR 1·71, 95% CI [1.16, 2.53]) but not for adults (HR 0.88, 95% CI [0.21, 3.69]).
Conclusion: Among children there was an increase in the hazard of ARI caused by non-influenza respiratory pathogens post-influenza vaccination compared to unvaccinated children during the same period. Potential mechanisms for this association warrant further investigation. Future research could investigate whether medical decision-making surrounding influenza vaccination may be improved by acknowledging patient experiences, counseling regarding different types of ARI, and correcting the misperception that all ARI occurring after vaccination are caused by influenza.
Keywords: Acute respiratory illness; Belief; Influenza; Influenza vaccine; Misperceptions.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
Similar articles
-
Acute respiratory illness in patients with COPD and the effectiveness of influenza vaccination: a randomized controlled study.Chest. 2004 Jun;125(6):2011-20. doi: 10.1378/chest.125.6.2011. Chest. 2004. PMID: 15189916 Clinical Trial.
-
Cohort profile: China respiratory illness surveillance among pregnant women (CRISP), 2015-2018.BMJ Open. 2018 Apr 28;8(4):e019709. doi: 10.1136/bmjopen-2017-019709. BMJ Open. 2018. PMID: 29705756 Free PMC article.
-
Influenza vaccination coverage and effectiveness in young children in Thailand, 2011-2013.Influenza Other Respir Viruses. 2015 Mar;9(2):85-93. doi: 10.1111/irv.12302. Epub 2015 Jan 5. Influenza Other Respir Viruses. 2015. PMID: 25557920 Free PMC article.
-
Seasonal influenza vaccines.Curr Top Microbiol Immunol. 2009;333:43-82. doi: 10.1007/978-3-540-92165-3_3. Curr Top Microbiol Immunol. 2009. PMID: 19768400 Review.
-
Influenza burden, prevention, and treatment in asthma-A scoping review by the EAACI Influenza in asthma task force.Allergy. 2018 Jun;73(6):1151-1181. doi: 10.1111/all.13333. Epub 2018 Jan 26. Allergy. 2018. PMID: 29105786
Cited by
-
Annual flu shot: Does it help patients with COVID-19?Int J Clin Pract. 2021 Dec;75(12):e14901. doi: 10.1111/ijcp.14901. Epub 2021 Sep 27. Int J Clin Pract. 2021. PMID: 34547161 Free PMC article.
-
Influenza vaccination and respiratory virus interference among Department of Defense personnel during the 2017-2018 influenza season.Vaccine. 2020 Jan 10;38(2):350-354. doi: 10.1016/j.vaccine.2019.10.005. Epub 2019 Oct 10. Vaccine. 2020. PMID: 31607599 Free PMC article.
-
Harnessing the non-specific immunogenic effects of available vaccines to combat COVID-19.Hum Vaccin Immunother. 2021 Jun 3;17(6):1650-1661. doi: 10.1080/21645515.2020.1833577. Epub 2020 Nov 13. Hum Vaccin Immunother. 2021. PMID: 33185497 Free PMC article.
-
Vaccine- and natural infection-induced mechanisms that could modulate vaccine safety.Toxicol Rep. 2020;7:1448-1458. doi: 10.1016/j.toxrep.2020.10.016. Epub 2020 Oct 22. Toxicol Rep. 2020. PMID: 33110761 Free PMC article. Review.
-
Specific and Nonspecific Effects of Influenza Vaccines.Vaccines (Basel). 2024 Apr 5;12(4):384. doi: 10.3390/vaccines12040384. Vaccines (Basel). 2024. PMID: 38675766 Free PMC article. Review.
References
-
- Bhat-Schelbert K., Lin C.J., Matambanadzo A., Hannibal K., Nowalk M.P., Zimmerman R.K. Barriers to and facilitators of child influenza vaccine – perspectives from parents, teens, marketing and healthcare professionals. Vaccine. 2012;30(14):2448–2452. - PubMed
-
- Naleway A.L., Henkle E.M., Ball S. Barriers and facilitators to influenza vaccination and vaccine coverage in a cohort of health care personnel. Am J Infect Control. 2014;42(4):371–375. - PubMed
-
- Hollmeyer H.G., Hayden F., Poland G., Buchholz U. Influenza vaccination of health care workers in hospitals—a review of studies on attitudes and predictors. Vaccine. 2009;27(30):3935–3944. - PubMed
-
- Nyhan B., Reifler J. Does correcting myths about the flu vaccine work? An experimental evaluation of the effects of corrective information. Vaccine. 2015;33(3):459–464. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
