

Non-ST-Segment-Elevation Myocardial Infarction Among Patients With Chronic Kidney Disease: A Propensity Score-Matched Comparison of Percutaneous Coronary Intervention Versus Conservative Management
- PMID: 29525779
- PMCID: PMC5907556
- DOI: 10.1161/JAHA.117.007920
Non-ST-Segment-Elevation Myocardial Infarction Among Patients With Chronic Kidney Disease: A Propensity Score-Matched Comparison of Percutaneous Coronary Intervention Versus Conservative Management
Abstract
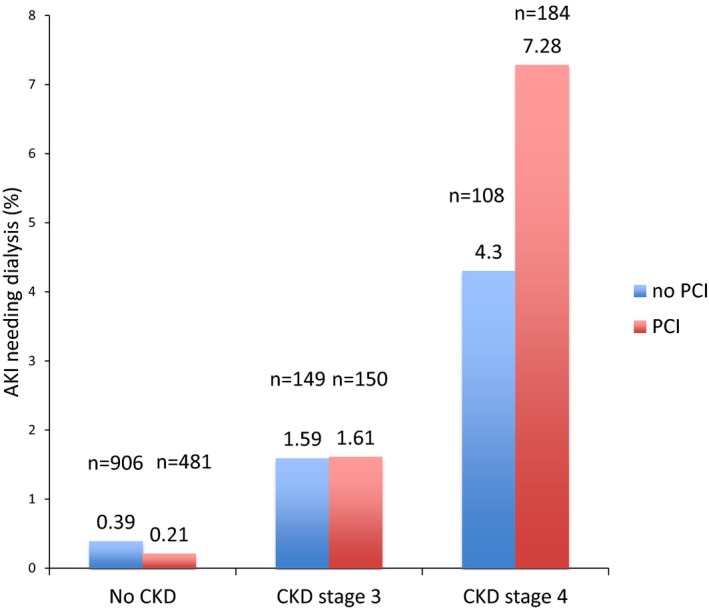
Background: Chronic kidney disease (CKD) remains an independent predictor of cardiovascular morbidity and mortality. CKD complicates referral for percutaneous coronary intervention (PCI) in non-ST-segment-elevation myocardial infarction (NSTEMI) patients because of the risk for acute kidney injury and the need for dialysis, with American College of Cardiology/American Heart Association guidelines underscoring the limited data on these patients.
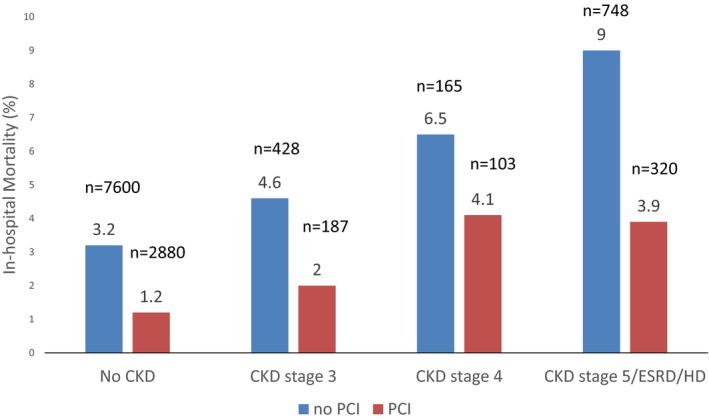
Methods and results: Using the National Inpatient Sample to analyze hospitalizations in the United States from 2004 to 2014, we sought to assess PCI utilization and in-hospital outcomes in NSTEMI admissions with CKD. NSTEMI admissions were identified by International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) code 410.7. CKD admissions were identified by ICD-9-CM code 585. Propensity score-matched cohorts of patients with NSTEMI were matched for age, sex, comorbidities, race, median household income, primary payer status, and hospital characteristics. Of 4 488 795 hospitalizations for NSTEMI, 31% underwent PCI. Overall, 89% of admissions had no CKD. In addition, 32% of NSTEMI admissions with no CKD and 23%, 14%, and 22% with CKD stages 3, 4, and 5 underwent PCI, respectively. Hospitalized NSTEMI patients with CKD stages 4 and 5 had 41% and 20% less likelihood, respectively, of undergoing PCI compared with those with no CKD. Among hospitalized NSTEMI patients with no CKD or CKD stage 3, 4, or 5, PCI-treated groups had 63%, 57%, 39%, and 59% lower likelihood, respectively, of all-cause, in-hospital mortality compared with propensity score-matched medically managed groups.
Conclusions: PCI use decreased among hospitalized NSTEMI patients as CKD severity increased, and all-cause, in-hospital mortality was greater for NSTEMI patients admitted with more severe CKD regardless of treatment strategy.
Keywords: acute coronary syndrome; chronic kidney disease.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Mehran R, Nikolsky E, Lansky AJ, Kirtane AJ, Kim YH, Feit F, Manoukian S, Moses JW, Ebrahimi R, Ohman EM, White HD, Pocock SJ, Dangas GD, Stone GW. Impact of chronic kidney disease on early (30‐day) and late (1‐year) outcomes of patients with acute coronary syndromes treated with alternative antithrombotic treatment strategies: an ACUITY (Acute Catheterization and Urgent Intervention Triage strategY) substudy. JACC Cardiovasc Interv. 2009;2:748–757. - PubMed
-
- Anavekar NS, McMurray JJ, Velazquez EJ, Solomon SD, Kober L, Rouleau JL, White HD, Nordlander R, Maggioni A, Dickstein K, Zelenkofske S, Leimberger JD, Califf RM, Pfeffer MA. Relation between renal dysfunction and cardiovascular outcomes after myocardial infarction. N Engl J Med. 2004;351:1285–1295. - PubMed
-
- Herzog CA, Asinger RW, Berger AK, Charytan DM, Diez J, Hart RG, Eckardt KU, Kasiske BL, McCullough PA, Passman RS, DeLoach SS, Pun PH, Ritz E. Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int. 2011;80:572–586. - PubMed
-
- Damman P, Hirsch A, Windhausen F, Tijssen JG, de Winter RJ. 5‐year clinical outcomes in the ICTUS (Invasive versus Conservative Treatment in Unstable coronary Syndromes) trial a randomized comparison of an early invasive versus selective invasive management in patients with non‐ST‐segment elevation acute coronary syndrome. J Am Coll Cardiol. 2010;55:858–864. - PubMed
-
- de Winter RJ, Windhausen F, Cornel JH, Dunselman PH, Janus CL, Bendermacher PE, Michels HR, Sanders GT, Tijssen JG, Verheugt FW. Early invasive versus selectively invasive management for acute coronary syndromes. N Engl J Med. 2005;353:1095–1104. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
