

Predictive Value of the Sequential Organ Failure Assessment Score for Mortality in a Contemporary Cardiac Intensive Care Unit Population
- PMID: 29525785
- PMCID: PMC5907568
- DOI: 10.1161/JAHA.117.008169
Predictive Value of the Sequential Organ Failure Assessment Score for Mortality in a Contemporary Cardiac Intensive Care Unit Population
Abstract
Background: Optimal methods of mortality risk stratification in patients in the cardiac intensive care unit (CICU) remain uncertain. We evaluated the ability of the Sequential Organ Failure Assessment (SOFA) score to predict mortality in a large cohort of unselected patients in the CICU.
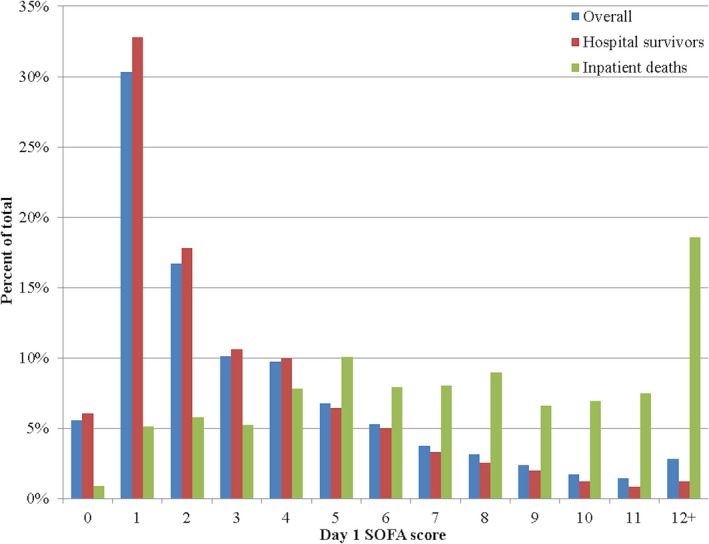
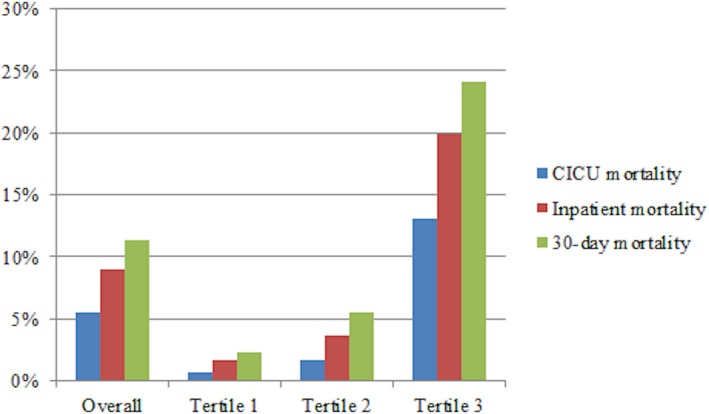
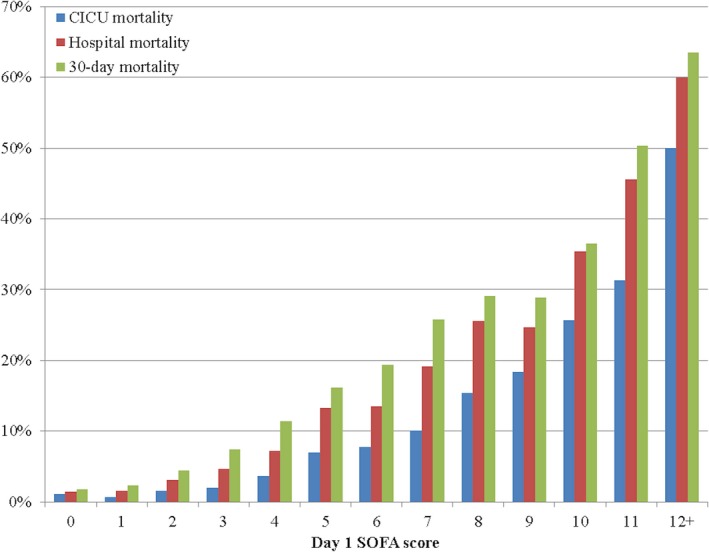
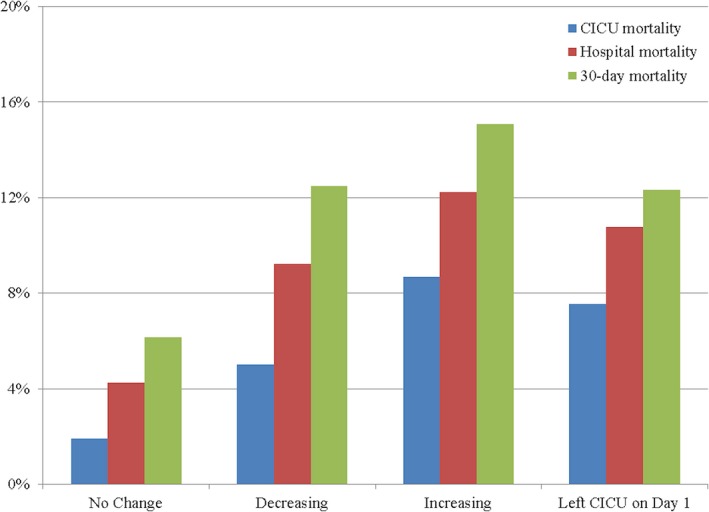
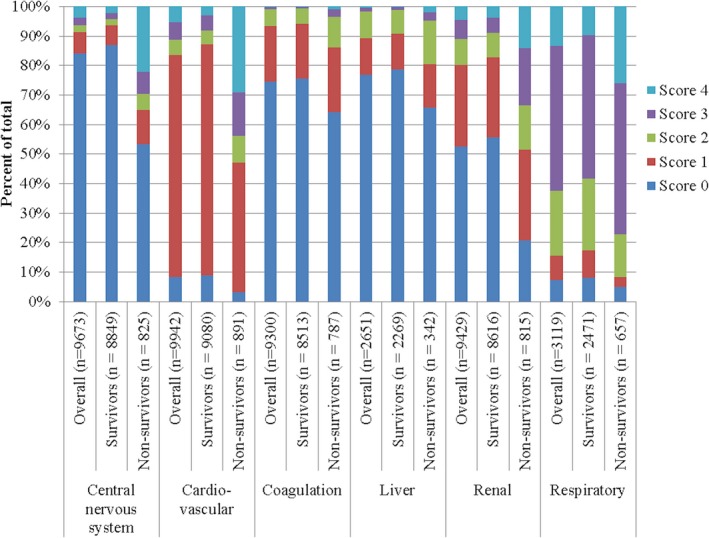
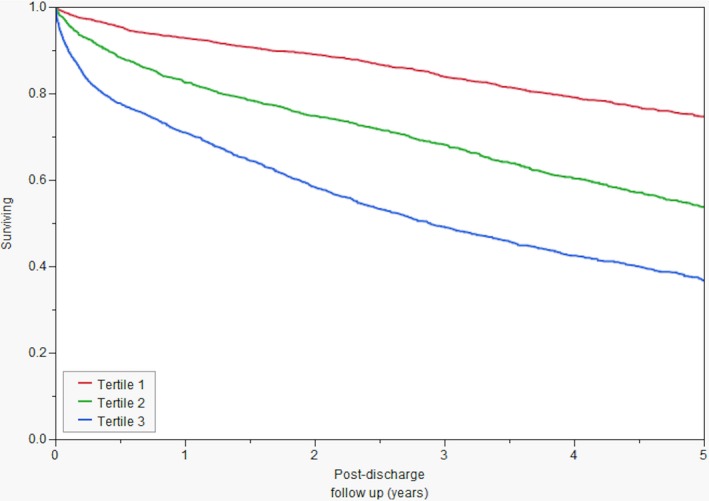
Methods and results: Adult patients admitted to the CICU from January 1, 2007, to December 31, 2015, at a single tertiary care hospital were retrospectively reviewed. SOFA scores were calculated daily, and Acute Physiology and Chronic Health Evaluation (APACHE)-III and APACHE-IV scores were calculated on CICU day 1. Discrimination of hospital mortality was assessed using area under the receiver-operator characteristic curve values. We included 9961 patients, with a mean age of 67.5±15.2 years; all-cause hospital mortality was 9.0%. Day 1 SOFA score predicted hospital mortality, with an area under the receiver-operator characteristic curve value of 0.83; area under the receiver-operator characteristic curve values were similar for the APACHE-III score, and APACHE-IV predicted mortality (P>0.05). Mean and maximum SOFA scores over multiple CICU days had greater discrimination for hospital mortality (P<0.01). Patients with an increasing SOFA score from day 1 and day 2 had higher mortality. Patients with day 1 SOFA score <2 were at low risk of mortality. Increasing tertiles of day 1 SOFA score predicted higher long-term mortality (P<0.001 by log-rank test).
Conclusions: The day 1 SOFA score has good discrimination for short-term mortality in unselected patients in the CICU, which is comparable to APACHE-III and APACHE-IV. Advantages of the SOFA score over APACHE include simplicity, improved discrimination using serial scores, and prediction of long-term mortality.
Keywords: Acute Physiology and Chronic Health Evaluation score; Sequential Organ Failure Assessment score; cardiac critical care; cardiac intensive care unit; critical care; intensive cardiac care unit; intensive care unit; mortality; risk prediction.
© 2018 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley.
Figures
References
-
- Killip T III, Kimball JT. Treatment of myocardial infarction in a coronary care unit: a two year experience with 250 patients. Am J Cardiol. 1967;20:457–464. - PubMed
-
- Katz JN, Shah BR, Volz EM, Horton JR, Shaw LK, Newby LK, Granger CB, Mark DB, Califf RM, Becker RC. Evolution of the coronary care unit: clinical characteristics and temporal trends in healthcare delivery and outcomes. Crit Care Med. 2010;38:375–381. - PubMed
-
- Katz JN, Minder M, Olenchock B, Price S, Goldfarb M, Washam JB, Barnett CF, Newby LK, van Diepen S. The genesis, maturation, and future of critical care cardiology. J Am Coll Cardiol. 2016;68:67–79. - PubMed
-
- Morrow DA, Fang JC, Fintel DJ, Granger CB, Katz JN, Kushner FG, Kuvin JT, Lopez‐Sendon J, McAreavey D, Nallamothu B, Page RL II, Parrillo JE, Peterson PN, Winkelman C; American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation, Council on Clinical Cardiology, Council on Cardiovascular Nursing, and Council on Quality of Care and Outcomes Research . Evolution of critical care cardiology: transformation of the cardiovascular intensive care unit and the emerging need for new medical staffing and training models: a scientific statement from the American Heart Association. Circulation. 2012;126:1408–1428. - PubMed
-
- Casella G, Cassin M, Chiarella F, Chinaglia A, Conte MR, Fradella G, Lucci D, Maggioni AP, Pirelli S, Scorcu G, Visconti LO; BLITZ‐3 Investigators . Epidemiology and patterns of care of patients admitted to Italian Intensive Cardiac Care units: the BLITZ‐3 registry. J Cardiovasc Med (Hagerstown). 2010;11:450–461. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
