

Fracture-pattern-related therapy concepts in distal humeral fractures
- PMID: 29527237
- PMCID: PMC5834588
- DOI: 10.1007/s11678-018-0442-8
Fracture-pattern-related therapy concepts in distal humeral fractures
Abstract
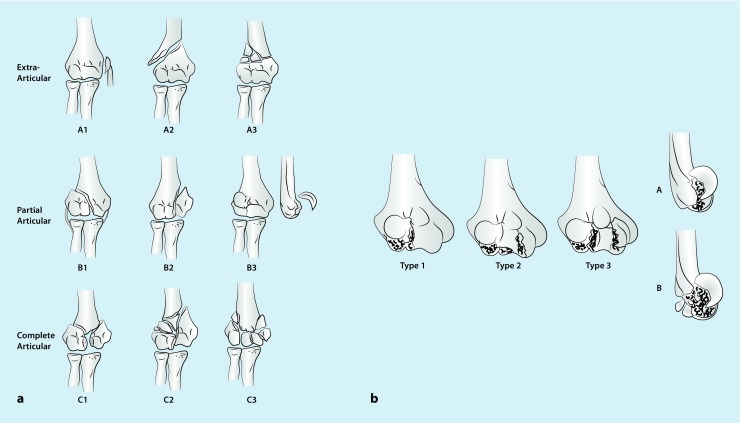
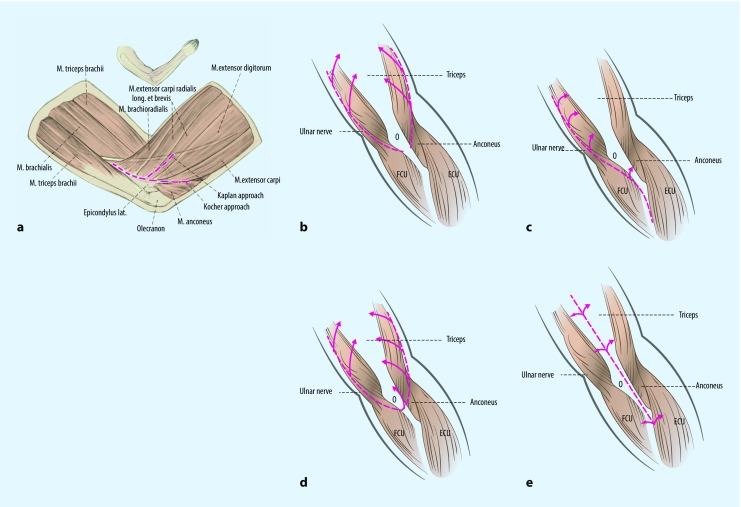
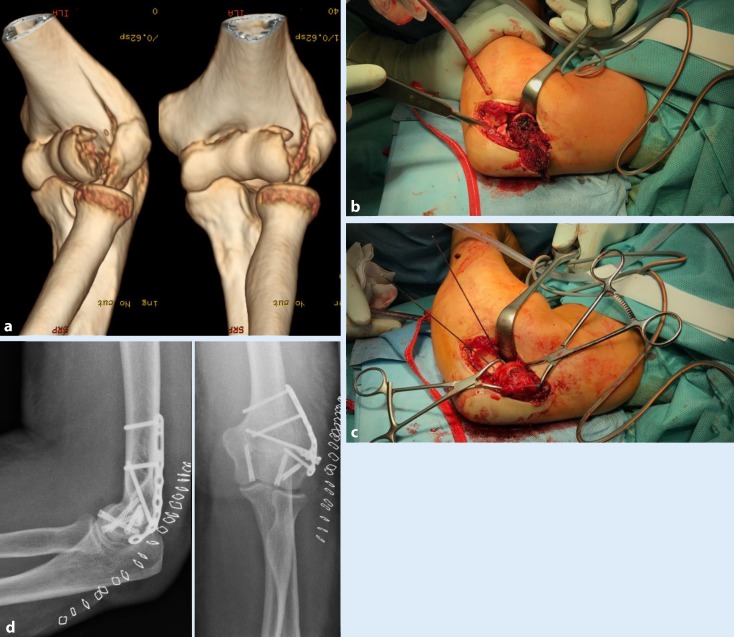
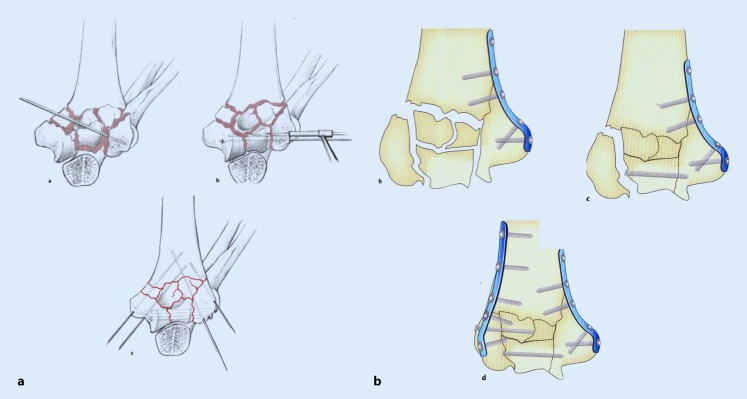
Around one third of humeral fractures and 2-6% of all fractures occur to the distal part of the humerus. There is a bimodal distribution differentiating between young male patients with high-energy and elderly female patients with low-energy trauma related to osteoporosis. The AO classification and Dubberley subclassification are used in daily routine. Most fractures are diagnosed on radiographs. For further evaluation, three-dimensional computed tomography is recommended, especially for comminuted or complex fractures. Owing to the long immobilization and resultant poor functional outcome, conservative treatment is followed for inoperable patients. The operative approach and osteosynthesis depend on the fracture pattern. In A1 avulsion fractures, open reduction and screw fixation are recommended. In A2/A3 fractures, a triceps-sparing approach following a 90° double-plate construction (radial dorsal/ulnar lateral) with locking plates is favored. Partial articular B1/B2 fractures are exposed via a medial or lateral approach using unilateral locking plates to stabilize the medial/lateral column. Coronal shear fractures (B3) are classified after Dubberley and are treated via an extended Kocher approach and headless compression screws in anteroposterior direction. If there is a further posterior comminution or a lateral column fragment, stabilization is needed for the lateral/medial column with a precontoured locking plate. In solely articular fracture patterns, a dorsal approach with either a 90° or 180° double-plate construction is advised. If a reconstruction is not possible owing to fracture complexity or bone quality, total elbow arthroplasty is a viable option. However, lifelong limitation in weight-bearing up to 5 kg, limited longevity, and the potential for complicated revision surgery should be considered.
Die distale Humerusfraktur stellt ein Drittel aller Humerusfrakturen und 2–6 % aller Frakturen dar. Dabei sind primär 2 Patientenkollektive zu unterscheiden: Männer zwischen 12–19 Jahren durch Hochrasanztraumata und Frauen über 80 Jahre mit osteoporotischer Knochenstruktur durch Niedrigenergietraumata. Im klinischen Alltag hat sich neben der AO-Klassifikation die Subklassifikation von frontalen Abscherfrakturen nach Dubberley als praktikabel erwiesen. Bereits im konventionellen Röntgenbild lässt sich ein Großteil der Frakturen erkennen. Zur exakten Klassifikation und Therapieplanung hat sich die Computertomographie mit dreidimensionaler Rekonstruktion insbesondere bei mehrfragmentären und komplexen Frakturen bewährt. Aufgrund längerer Immobilisation und häufig hieraus resultierenden deutlichen funktionellen Einbußen bleibt die konservative Therapie inoperablen Patienten vorbehalten. Der operative Zugangsweg und das jeweilige Osteosyntheseverfahren sind frakturspezifisch zu wählen. Dabei haben sich neben der mono-/bikondylären winkelstabilen Plattenosteosynthese die Schraubenosteosynthese und neuerdings kopflose Kompressionsschrauben mit Doppelgewinde durchgesetzt. Epikondyläre A1-Frakturen werden mittels Schraubenosteosynthese versorgt. Für metaphysäre A2-/A3-Frakturen wird ein den Streckapparat schonender paratrizipitaler Zugang und eine Doppelplattenosteosynthese in 90°-Technik favorisiert. Partiell artikuläre B1- und B2-Frakturen können entsprechend ihrer Lage entweder über einen radialen oder medialen Zugang erreicht und mittels einseitiger winkelstabiler Plattenosteosynthese versorgt werden. Frontale Abscherfrakturen (B3) werden mit einem erweiterten lateralen Zugang nach Kocher, mittels kopfloser Doppelgewindekompressionsschrauben und bei radialem/ulnarem Pfeiler mit additiver winkelstabiler Plattenosteosynthese fixiert. Vollständige artikuläre Frakturen (C1–C3) werden von dorsal dargestellt und je nach Wahl des Operateurs in winkelstabiler 90°-/180°-Doppelplattenosteosynthese fixiert. Ist eine Rekonstruktion unmöglich, stellt eine prothetische Versorgung des Ellenbogens eine Alternative da, wobei die lebenslange Limitierung der Belastbarkeit von 5 kg und limitierte Standzeiten sowie mögliche komplizierte Revisionsoperationen zu berücksichtigen sind.
Keywords: AO classification; Double plate constructions; Dubberley sub classification; Headless compression screws; Lateral approach; Total elbow arthroplasty.
Conflict of interest statement
Compliance with ethical guidelinesH. Lill is consultant with Arthrex (Karlsfeld, Deutschland) and DePuy Synthes (Umkirch, Deutschland). R.-O. Dey Hazra, G. Jensen, J. Imrecke, and A. Ellwein declare that they have no competing interests. This article does not contain any studies with human participants or animals performed by any of the authors.
Figures



Similar articles
-
Biomechanical evaluation of a transcondylar screw from the dorsolateral plate support on the stabilization of orthogonal plate configuration in distal humeral fracture.Injury. 2019 Feb;50(2):256-262. doi: 10.1016/j.injury.2018.12.017. Epub 2018 Dec 16. Injury. 2019. PMID: 30579588
-
[Operative effect and treatment strategies for the low distal humerus fracture].Zhonghua Wai Ke Za Zhi. 2020 Mar 1;58(3):213-219. doi: 10.3760/cma.j.issn.0529-5815.2020.03.009. Zhonghua Wai Ke Za Zhi. 2020. PMID: 32187925 Chinese.
-
Internal fixation of proximal humerus fractures using the locking proximal humerus plate.Oper Orthop Traumatol. 2005 Feb;17(1):25-50. doi: 10.1007/s00064-005-1120-8. Oper Orthop Traumatol. 2005. PMID: 16007377 Clinical Trial. English, German.
-
Management of distal humeral coronal shear fractures.World J Clin Cases. 2015 May 16;3(5):405-17. doi: 10.12998/wjcc.v3.i5.405. World J Clin Cases. 2015. PMID: 25984515 Free PMC article. Review.
-
[Reduction techniques for minimally invasive stabilization of proximal humeral fractures].Oper Orthop Traumatol. 2019 Feb;31(1):63-80. doi: 10.1007/s00064-018-0586-0. Epub 2019 Jan 25. Oper Orthop Traumatol. 2019. PMID: 30683977 Review. German.
Cited by
-
Post-Surgical Ulnar Nerve Neuropathy in Distal Humerus Fractures: Comparison Between In Situ Decompression and Anterior Subcutaneous Transposition.J Clin Med. 2025 Apr 5;14(7):2490. doi: 10.3390/jcm14072490. J Clin Med. 2025. PMID: 40217939 Free PMC article.
-
Hemiarthroplasty versus open reduction internal fixation for intra-articular distal humerus fractures in older patients.Shoulder Elbow. 2023 Feb;15(1):83-92. doi: 10.1177/17585732221093004. Epub 2022 Apr 18. Shoulder Elbow. 2023. PMID: 36895603 Free PMC article.
-
Development of three-dimensional preoperative planning system for the osteosynthesis of distal humerus fractures.Biomed Eng Online. 2020 Jul 13;19(1):56. doi: 10.1186/s12938-020-00801-3. Biomed Eng Online. 2020. PMID: 32660498 Free PMC article.
-
Use of a 5-item modified Fragility Index for risk stratification in patients undergoing surgical management of distal humerus fractures.JSES Int. 2021 Sep 17;5(6):1111-1118. doi: 10.1016/j.jseint.2021.07.016. eCollection 2021 Nov. JSES Int. 2021. PMID: 34766092 Free PMC article.
-
Functional Outcome and Inflammatory Response of Patients with Extra-Articular Distal Humeral Fractures following Implantation of Anatomically Precontoured Locking Compression Plates through a Posterior Approach.Evid Based Complement Alternat Med. 2021 Jul 28;2021:2426298. doi: 10.1155/2021/2426298. eCollection 2021. Evid Based Complement Alternat Med. 2021. Retraction in: Evid Based Complement Alternat Med. 2023 Jun 21;2023:9802457. doi: 10.1155/2023/9802457. PMID: 34367298 Free PMC article. Retracted.
References
-
- Müller ME, Nazarian S, Koch P, Schatzker J. The comprehensive classification of fractures of long bones. Heidelberg: Springer; 1990.
-
- Dubberley JH, Faber KJ, Macdermid JC, et al. Outcome after open reduction and internal fixation of capitellar and trochlear fractures. J Bone Joint Surg Am. 2006;88:46–54. - PubMed
-
- Doornberg J, Ring D, Jupiter JB. Effective treatment of fracture-dislocations of the olecranon requires a stable trochlear notch. Clin Orthop Relat Res. 2004 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources