

mCME project V.2.0: randomised controlled trial of a revised SMS-based continuing medical education intervention among HIV clinicians in Vietnam
- PMID: 29527350
- PMCID: PMC5841494
- DOI: 10.1136/bmjgh-2017-000632
mCME project V.2.0: randomised controlled trial of a revised SMS-based continuing medical education intervention among HIV clinicians in Vietnam
Abstract
Background: Continuing medical education (CME) is indispensable, but costs are a barrier. We tested the effectiveness of a novel mHealth intervention (mCME V.2.0) promoting CME among Vietnamese HIV clinicians.
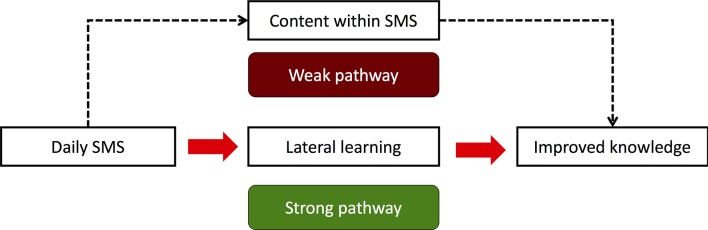
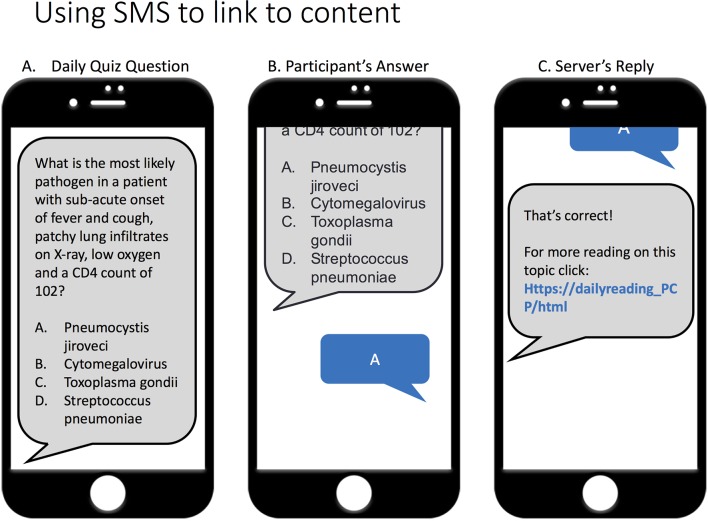
Methods: We enrolled HIV clinicians from three provinces near Hanoi. The 6-month intervention consisted of (1) daily short message service multiple-choice quiz questions, (2) daily linked readings, (3) links to online CME courses and (4) feedback messages describing the performance of the participant relative to the group. Control participants had equal access to the online CME courses. Our primary endpoint was utilisation of the online CME courses; secondary endpoints were self-study behaviour, performance on a standardised medical exam and job satisfaction.
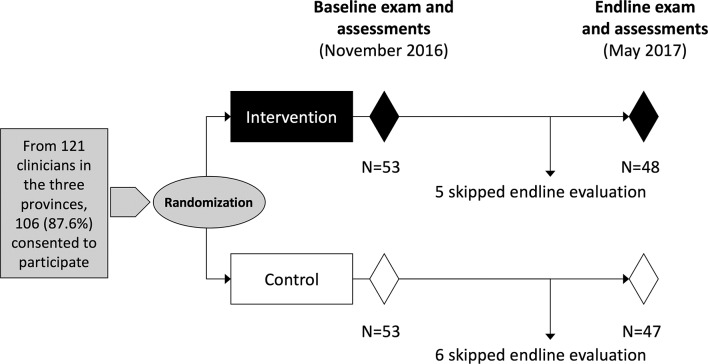
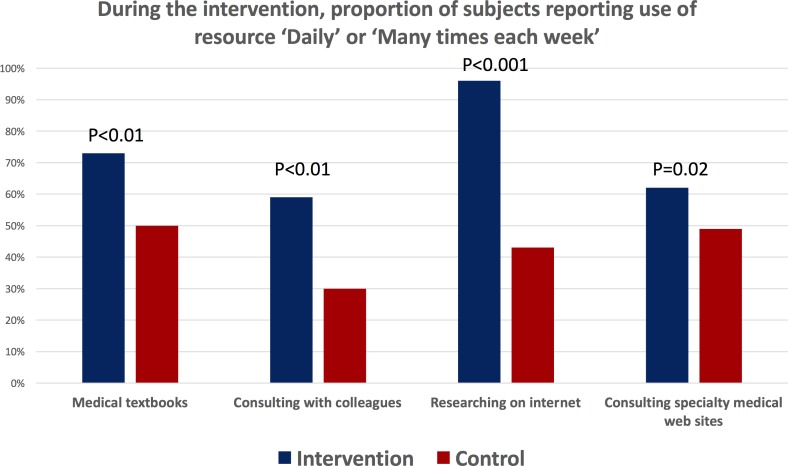
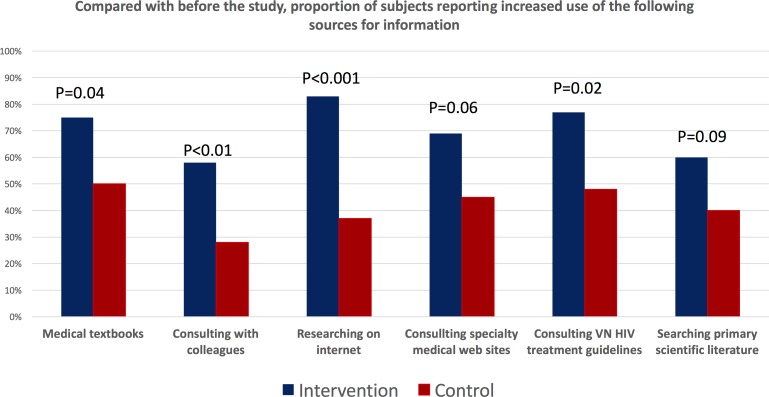
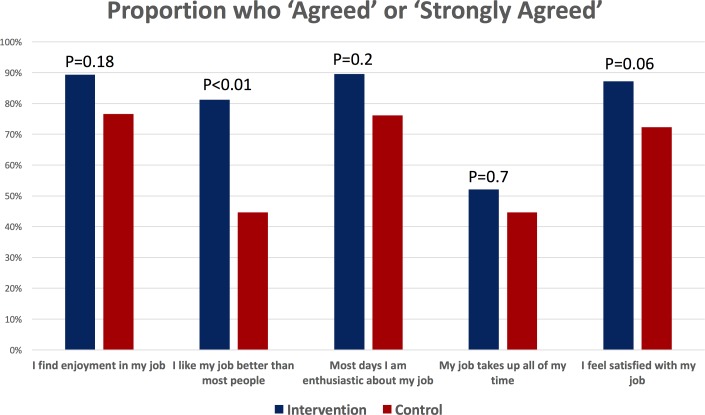
Results: From 121 total HIV clinicians in the three provinces, 106 (87.6%) enrolled, and 48/53 intervention (90%) and 47/53 control (89%) participants completed the endline evaluations. Compared with controls, intervention participants were more likely to use the CME courses (risk ratio (RR) 2.3, 95% CI 1.4 to 3.8, accounting for 83% of course use (P<0.001)). Intervention participants increased self-study behaviours over controls in terms of use of medical textbooks (P<0.01), consulting with colleagues (P<0.01), searching on the internet (P<0.001), using specialist websites (P=0.02), consulting the Vietnam HIV/AIDS treatment guidelines (P=0.02) and searching the scientific literature (P=0.09). Intervention participants outperformed controls on the exam (+23% vs +12% score gains, P=0.05) and had higher job satisfaction.
Conclusion: The mCME V.2.0 intervention improved self-study behaviour, medical knowledge and job satisfaction. This approach has potential for expansion in Vietnam and similar settings.
Trial registration number: NCT02381743.
Keywords: health education and promotion; health policy; public health; randomised control trial.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Costs and Cost-Effectiveness of mCME Version 2.0: An SMS-Based Continuing Medical Education Program for HIV Clinicians in Vietnam.Glob Health Sci Pract. 2022 Aug 30;10(4):e2200008. doi: 10.9745/GHSP-D-22-00008. Print 2022 Aug 30. Glob Health Sci Pract. 2022. PMID: 36041848 Free PMC article. Clinical Trial.
-
Motivating HIV Providers in Vietnam to Learn: A Mixed-Methods Analysis of a Mobile Health Continuing Medical Education Intervention.JMIR Med Educ. 2019 Apr 18;5(1):e12058. doi: 10.2196/12058. JMIR Med Educ. 2019. PMID: 30998220 Free PMC article.
-
The mCME Project: A Randomized Controlled Trial of an SMS-Based Continuing Medical Education Intervention for Improving Medical Knowledge among Vietnamese Community Based Physicians' Assistants.PLoS One. 2016 Nov 18;11(11):e0166293. doi: 10.1371/journal.pone.0166293. eCollection 2016. PLoS One. 2016. PMID: 27861516 Free PMC article. Clinical Trial.
-
Unpacking the "Black Box": How an SMS-Based Continuing Medical Education Intervention Improved Medical Knowledge Among HIV Clinicians in Vietnam.Glob Health Sci Pract. 2018 Dec 27;6(4):668-679. doi: 10.9745/GHSP-D-18-00298. Print 2018 Dec 27. Glob Health Sci Pract. 2018. PMID: 30591575 Free PMC article.
-
Collaborative online learning: a new approach to distance CME.Acad Med. 2002 Sep;77(9):928-9. Acad Med. 2002. PMID: 12228097 Review.
Cited by
-
Patient-Centered Care: Transforming the Health Care System in Vietnam With Support of Digital Health Technology.J Med Internet Res. 2021 Jun 4;23(6):e24601. doi: 10.2196/24601. J Med Internet Res. 2021. PMID: 34085939 Free PMC article.
-
Costs and Cost-Effectiveness of mCME Version 2.0: An SMS-Based Continuing Medical Education Program for HIV Clinicians in Vietnam.Glob Health Sci Pract. 2022 Aug 30;10(4):e2200008. doi: 10.9745/GHSP-D-22-00008. Print 2022 Aug 30. Glob Health Sci Pract. 2022. PMID: 36041848 Free PMC article. Clinical Trial.
-
Use of eHealth for HIV Medical Education: a Narrative Review.Curr HIV/AIDS Rep. 2021 Jun;18(3):247-260. doi: 10.1007/s11904-021-00553-2. Epub 2021 Apr 5. Curr HIV/AIDS Rep. 2021. PMID: 33817768 Review.
-
Motivating HIV Providers in Vietnam to Learn: A Mixed-Methods Analysis of a Mobile Health Continuing Medical Education Intervention.JMIR Med Educ. 2019 Apr 18;5(1):e12058. doi: 10.2196/12058. JMIR Med Educ. 2019. PMID: 30998220 Free PMC article.
-
Implementing the mobile continuing medical education (mCME) project in Vietnam: making it work and sharing lessons learned.Mhealth. 2019 Feb 25;5:7. doi: 10.21037/mhealth.2019.02.01. eCollection 2019. Mhealth. 2019. PMID: 30976599 Free PMC article.
References
-
- Gill CJ, Le Ngoc B, Halim N, et al. . The mCME Project: a randomized controlled trial of an SMS-Based continuing medical education intervention for improving medical knowledge among vietnamese community based physicians’ assistants. PLoS One 2016;11:e0166293 10.1371/journal.pone.0166293 - DOI - PMC - PubMed
-
- Glanz K, Rimer B, Lewis F. Health behavior and health education: theory, research and practice. San Francisco: Wiley & Sons, 2002.
-
- Sabin LL, Larson Williams A, Le BN, et al. . Benefits and limitations of text messages to stimulate higher learning among community providers: participants’ views of an mhealth intervention to support continuing medical education in Vietnam. Glob Health Sci Pract 2017;5:261–73. 10.9745/GHSP-D-16-00348 - DOI - PMC - PubMed
-
- Thompson ER, Phua FTT. A Brief Index of Affective Job Satisfaction. Group Organ Manag 2012;37:275–307. 10.1177/1059601111434201 - DOI
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical