

Nursing review of spinal meningiomas
- PMID: 29527399
- PMCID: PMC5838844
- DOI: 10.4103/sni.sni_408_17
Nursing review of spinal meningiomas
Abstract
Background: Spinal meningiomas are found in patients typically between the ages of 75 and 84: some report the average age to be 50. They occur with an incidence of approximately 1000 patients per year in the US, are mostly single (90%) rather than multiple (10%), and arise from the spinal meninges (arachnoid/dura). Tumors are typically posterior/posterolateral (70%) in location, leaving the remaining 30% in the anterior/anterolateral spinal canal. They produce symptoms and signs of radiculopathy (nerve root) and/or myelopathy (cord compression) depending on their site of origin.
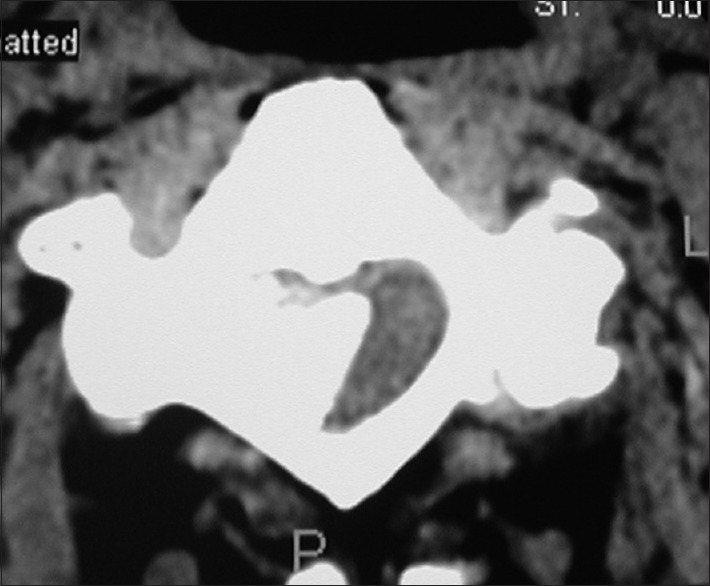
Methods: Meningiomas may be single/sporadic (90%) or multifocal. They may arise primarily/spontaneously, can be radiation-induced, or associated with neurofibromatosis. They are found most frequently in females vs. males in up to a 3.4:1 ratio, occur predominantly in the thoracic spine. They are found in decreasing order in the cervical and lumbar spinal canals. The diagnosis of a meningioma is based on magnetic resonance (MR) studies, where tumors are isointense on T1 weighted MR, and hyperintense onf T2-weighted MR images; they also typically uniformly enhance with Gd-DTPA. On computed tomography (CT) examinations, they are usually characterized as calcified/hyperdense.
Results: The neurological deficits resulting from meningiomas and the rapidity of symptom/sign progression dictate whether they are treated surgically or nonsurgically. Management choices include; stereotactic radiation therapy only, and/or in combination with varied surgical resection techniques.
Conclusions: The majority of benign spinal cord tumors are meningiomas (40%) that are predominantly found in the thoracic spine in middle-aged females. Tumor levels (e.g. in descending order cervical, thoracic, lumbar), and their location (e.g. anterior/anterolateral 30%; dorsal/dorsolateral 70%) best determine whether nonoperative, operative, and/or operative intervention combined with routine vs. stereotactic radiosurgery are warranted.
Keywords: CT; Diagnostic studies; MR; locations; prognosis; routine radiation; spinal meningiomas; stereotactic radiosurgery/Cyberknife; surgical techniques; tumors.
Conflict of interest statement
There are no conflicts of interest.
Figures









References
-
- Bayoumi AB, Laviv Y, Yokus B, Efe IE, Toktas ZO, Kilic T, et al. Proposal of a new radiological classification system for spinal meningiomas as a descriptive tool and surgical guide. Clin Neurol Neurosurg. 2017;162:118–26. - PubMed
-
- Kshettry VR, Hsieh JK, Ostrom QT, Kruchko C, Benzel EC, Barnholtz-Sloan JS. Descriptive Epidemiology of Spinal Meningiomas in the United States. Spine (Phila Pa 1976) 2015;40:E886–9. - PubMed
-
- Mawrin C, Perry A. Pathological classification and molecular genetics of meningiomas. J Neurooncol. 2010;99:379–91. - PubMed
-
- Roux FX, Nataf F, Pinaudeau M, Borne G, Devaux B, Meder JF. Intraspinal meningiomas: Review of 54 cases with discussion of poor prognosis factors and modern therapeutic management. Surg Neurol. 1996;46:458–63. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials