

The potential value of probabilistic tractography-based for MR-guided focused ultrasound thalamotomy for essential tremor
- PMID: 29527503
- PMCID: PMC5842733
- DOI: 10.1016/j.nicl.2017.12.018
The potential value of probabilistic tractography-based for MR-guided focused ultrasound thalamotomy for essential tremor
Abstract
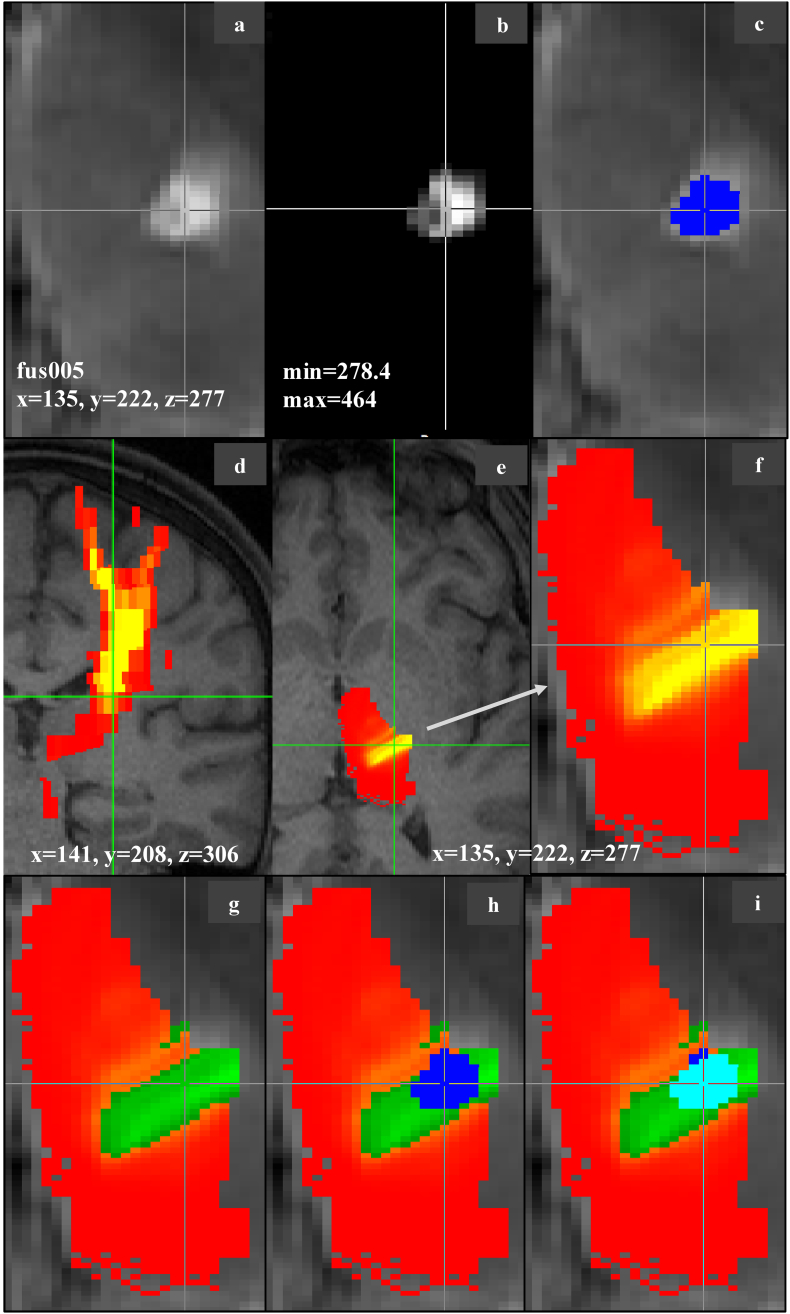
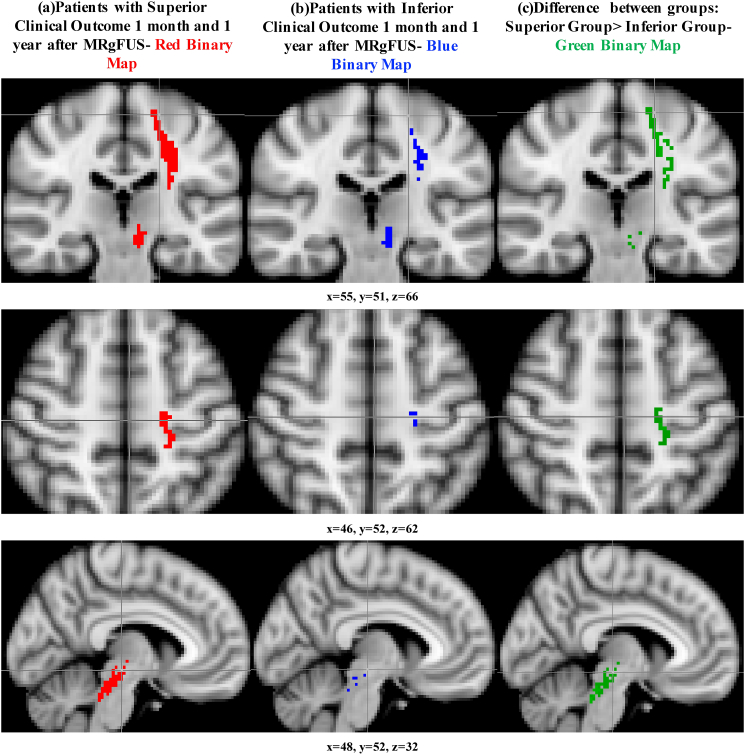
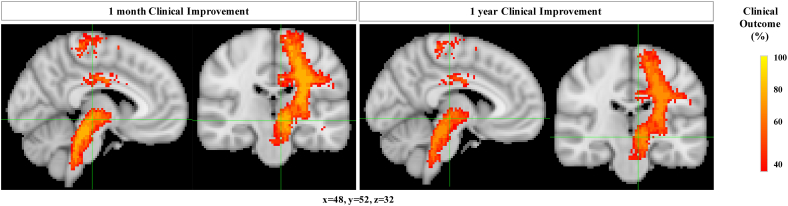
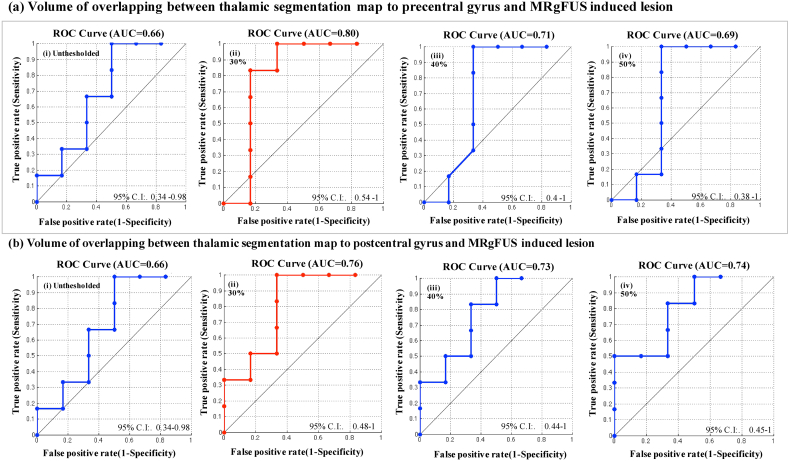
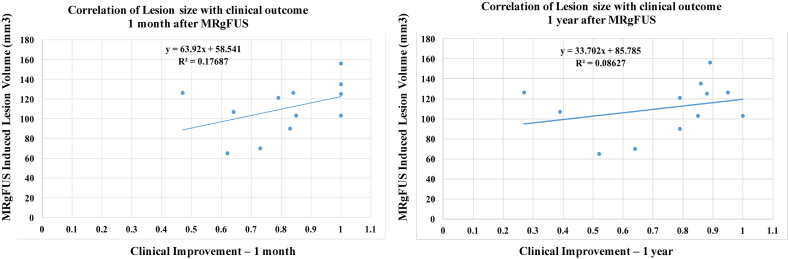
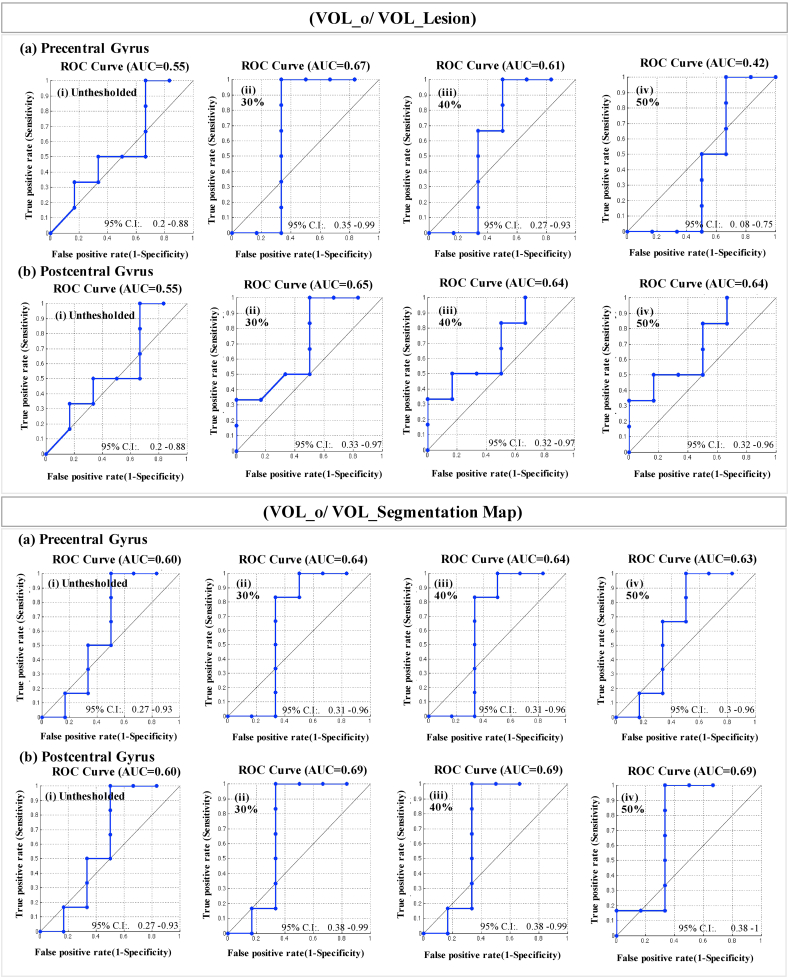
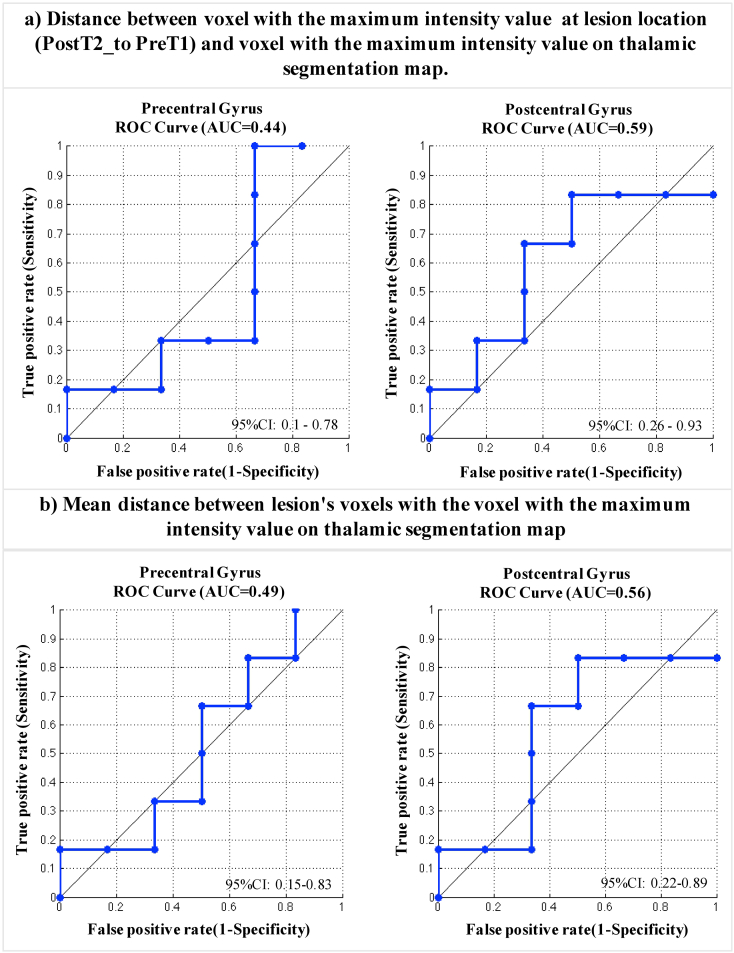
Magnetic Resonance-guided Focused UltraSound (MRgFUS) offers an incisionless approach to treat essential tremor (ET). Due to lack of evident internal anatomy on traditional structural imaging, indirect targeting must still be used to localize the lesion. Here, we investigate the potential predictive value of probabilistic tractography guided thalamic targeting by defining how tractography-defined targets, lesion size and location, and clinical outcomes interrelate. MR imaging and clinical outcomes from 12 ET patients that underwent MRgFUS thalamotomy in a pilot study at the University of Virginia were evaluated in this analysis. FSL was used to evaluate each patient's voxel-wise thalamic connectivity with FreeSurfer generated pre- and post-central gyrus targets, to generate thalamic target maps. Using Receiver Operating Characteristic curves, the overlap between these thalamic target maps and the MRgFUS lesion was systematically evaluated relative to clinical outcome. To further define the connectivity characteristics of effective MRgFUS thalamotomy lesions, we evaluated whole brain probabilistic tractography of lesions (using post-treatment imaging to define the lesion pre-treatment diffusion tensor MRI). The structural connectivity difference was explored between subjects with the best clinical outcome relative to all others. Ten of twelve patients presented high percentage of overlapping between connectivity-based thalamic segmentation maps and lesion area. The improvement of clinical score was predicted (AUC: 0.80) using the volume of intersection between the thalamic target (precentral gyrus) map and MRgFUS induced lesion as feature. The main structural differences between those with different magnitudes of response were observed in connectivity to the pre- and post-central gyri and brainstem/cerebellum. MRgFUS thalamotomy lesions characterized by strong structural connectivity to precentral gyrus demonstrated better responses in a cohort of patients treated with MRgFUS for ET. The intersection between lesion and thalamic-connectivity maps to motor - sensory targets proved to be effective in predicting the response to the therapy. These imaging techniques can be used to increase the efficacy and consistency of outcomes with MRgFUS and potentially shorten treatment times by identifying optimal targets in advance of treatment.
Keywords: Magnetic resonance imaging-guided focused ultrasound; Tractography; Tremor.
Figures
Similar articles
-
Quantitative Tractography-Based Evaluations in Essential Tremor Patients after MRgFUS Thalamotomy.Mov Disord Clin Pract. 2024 Dec;11(12):1516-1529. doi: 10.1002/mdc3.14219. Epub 2024 Oct 5. Mov Disord Clin Pract. 2024. PMID: 39367682 Free PMC article.
-
Clinical improvement associated with targeted interruption of the cerebellothalamic tract following MR-guided focused ultrasound for essential tremor.J Neurosurg. 2018 Aug;129(2):315-323. doi: 10.3171/2017.4.JNS162803. Epub 2017 Oct 20. J Neurosurg. 2018. PMID: 29053074
-
Four-tract probabilistic tractography technique for target selection in essential tremor treatment with magnetic resonance-guided focused ultrasound.Eur Radiol. 2024 Aug;34(8):5167-5178. doi: 10.1007/s00330-023-10431-7. Epub 2023 Nov 11. Eur Radiol. 2024. PMID: 37950079
-
3-T MR-guided focused ultrasound thalamotomy for tremor in patients with a cardiac pacemaker: case series and review of the literature.Neurosurg Focus. 2024 Sep 1;57(3):E5. doi: 10.3171/2024.6.FOCUS24171. Neurosurg Focus. 2024. PMID: 39217637 Review.
-
Comparison between deep brain stimulation and magnetic resonance-guided focused ultrasound in the treatment of essential tremor: a systematic review and pooled analysis of functional outcomes.J Neurol Neurosurg Psychiatry. 2020 Dec;91(12):1270-1278. doi: 10.1136/jnnp-2020-323216. Epub 2020 Oct 14. J Neurol Neurosurg Psychiatry. 2020. PMID: 33055140
Cited by
-
Improved Vim targeting for focused ultrasound ablation treatment of essential tremor: A probabilistic and patient-specific approach.Hum Brain Mapp. 2020 Dec;41(17):4769-4788. doi: 10.1002/hbm.25157. Epub 2020 Aug 6. Hum Brain Mapp. 2020. PMID: 32762005 Free PMC article.
-
Improving tremor response to focused ultrasound thalamotomy.Brain Commun. 2023 May 22;5(4):fcad165. doi: 10.1093/braincomms/fcad165. eCollection 2023. Brain Commun. 2023. PMID: 37533544 Free PMC article.
-
Longitudinal MR imaging after unilateral MR-guided focused ultrasound thalamotomy: clinical and radiological correlation.Front Neurol. 2023 Oct 6;14:1272425. doi: 10.3389/fneur.2023.1272425. eCollection 2023. Front Neurol. 2023. PMID: 37869137 Free PMC article.
-
Dosimetric Comparison of Dedicated Radiosurgery Platforms for the Treatment of Essential Tremor: Technical Report.Cureus. 2024 Apr 2;16(4):e57452. doi: 10.7759/cureus.57452. eCollection 2024 Apr. Cureus. 2024. PMID: 38699125 Free PMC article.
-
Connectivity-based segmentation of the thalamic motor region for deep brain stimulation in essential tremor: A comparison of deterministic and probabilistic tractography.Neuroimage Clin. 2024;41:103587. doi: 10.1016/j.nicl.2024.103587. Epub 2024 Feb 27. Neuroimage Clin. 2024. PMID: 38422832 Free PMC article.
References
-
- Alusi S.H., Aziz T.Z., Glickman S., Jahanshahi M., Stein J.F., Bain P.G. Stereotactic lesional surgery for the treatment of tremor in multiple sclerosis: a prospective case-controlled study. Brain. 2001;124:1576–1589. - PubMed
-
- Andersson J.L.R., Jenkinson M., Smith S. FMRIB Technical Report TR07JA2. vol. 22. Oxford Cent. Funct. Magn. Reson. Imaging Brain, Dep. Clin. Neurol. Oxford Univ.; Oxford, UK: 2007. Non-linear registration, aka spatial normalisation.
-
- Avecillas-Chasin J.M., Alonso-Frech F., Parras O., del Prado N., Barcia J.A. Assessment of a method to determine deep brain stimulation targets using deterministic tractography in a navigation system. Neurosurg. Rev. 2015;38:739–751. - PubMed
-
- Basser P.J., Özarslan E. second edition. Academic Press; San Diego: 2014. Chapter 1 - Introduction to Diffusion MR BT - Diffusion MRI; pp. 3–9.
-
- Behrens T.E.J., Woolrich M.W., Jenkinson M., Johansen-Berg H., Nunes R.G., Clare S., Matthews P.M., Brady J.M., Smith S.M. Characterization and propagation of uncertainty in diffusion-weighted MR imaging. Magn. Reson. Med. 2003;50:1077–1088. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
