

EUS-guided gastroenterostomy in management of benign gastric outlet obstruction
- PMID: 29527559
- PMCID: PMC5842065
- DOI: 10.1055/s-0043-123468
EUS-guided gastroenterostomy in management of benign gastric outlet obstruction
Erratum in
-
Erratum: EUS-guided gastroenterostomy in management of benign gastric outlet obstruction.Endosc Int Open. 2018 Mar;6(3):C3. doi: 10.1055/a-0747-0202. Epub 2018 Sep 20. Endosc Int Open. 2018. PMID: 30250872 Free PMC article.
Abstract
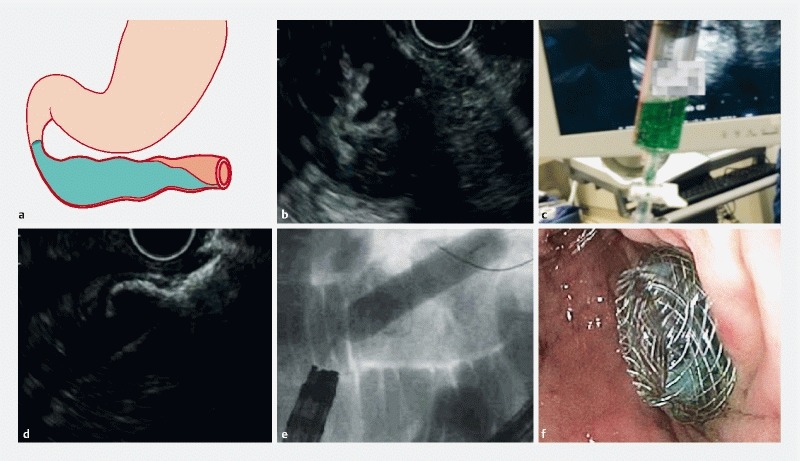
Background and study aims: Endoscopic ultrasound-guided gastroenterostomy (EUS-GE) in malignant gastric outlet obstruction (GOO) appears to be promising; however, its role in benign GOO is unclear. The aim of this study was to ascertain the clinical efficacy and safety of EUS-GE in benign GOO.
Patients and methods: This was an international retrospective series involving 5 tertiary centers. Consecutive patients who underwent EUS-GE between 1/2013 - 10/2016 for benign GOO were included. The primary endpoint was the rate of clinical success defined as ability to tolerate oral intake without vomiting. Secondary endpoints included technical success and rate of adverse events (AE).
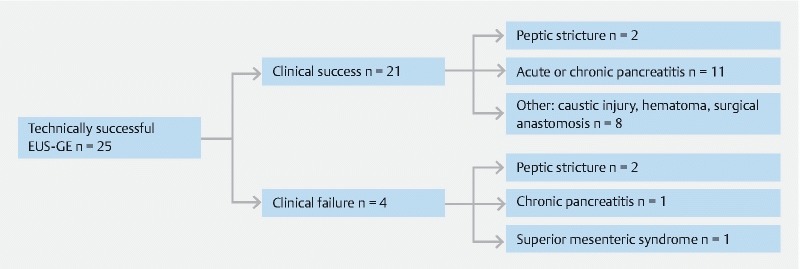
Results: Overall, 26 patients (46.2 % female; mean age 57.7 ± 13.9 years) underwent EUS-GE for benign GOO due to strictures from chronic pancreatitis (n = 11), surgical anastomosis (n = 6), peptic ulcer disease (n = 5), acute pancreatitis (n = 1), superior mesentery artery syndrome (n = 1), caustic injury (n = 1), and hematoma (n = 1). Technical success was achieved in 96.2 %. Dilation of the lumen apposing metal stent was performed in 13/25 (52 %) with a mean maximum diameter of 14.6 ± 1.0 mm. Mean procedure time was 44.6 ± 26.1 min. Clinical success was observed in 84.0 % with a mean time to oral intake of 1.4 ± 1.9 days and a median follow-up of 176.5 (IQR: 47 - 445.75) days. Rate of unplanned re-intervention was 4.8 %. 3 AE were noted including 2 misdeployed stents and 1 gastric leak needing surgical intervention following elective GE stent removal.
Conclusions: EUS-GE is a promising treatment for benign GOO. Larger and prospective data are needed to further validate this novel endoscopic technique in treating benign GOO of various etiologies.
Conflict of interest statement
Figures
References
-
- Committee ASoP . Banerjee S, Cash B D et al.The role of endoscopy in the management of patients with peptic ulcer disease. Gastrointest Endosc. 2010;71:663–668. - PubMed
-
- Paimela H, Tuompo P K, Perakyl T et al.Peptic ulcer surgery during the H2-receptor antagonist era: a population-based epidemiological study of ulcer surgery in Helsinki from 1972 to 1987. Br J Surg. 1991;78:28–31. - PubMed
-
- Johnson C D, Ellis H. Gastric outlet obstruction now predicts malignancy. Br J Surg. 1990;77:1023–1024. - PubMed
-
- Khullar S K, DiSario J A. Gastric outlet obstruction. Gastrointest Endosc Clin N Am. 1996;6:585–603. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical