

Potential lymphangiogenesis therapies: Learning from current antiangiogenesis therapies-A review
- PMID: 29528507
- PMCID: PMC6135718
- DOI: 10.1002/med.21496
Potential lymphangiogenesis therapies: Learning from current antiangiogenesis therapies-A review
Abstract
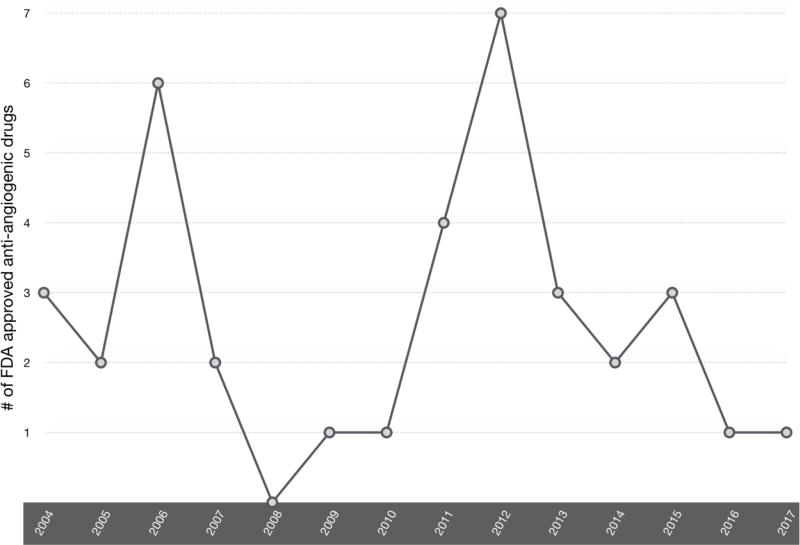
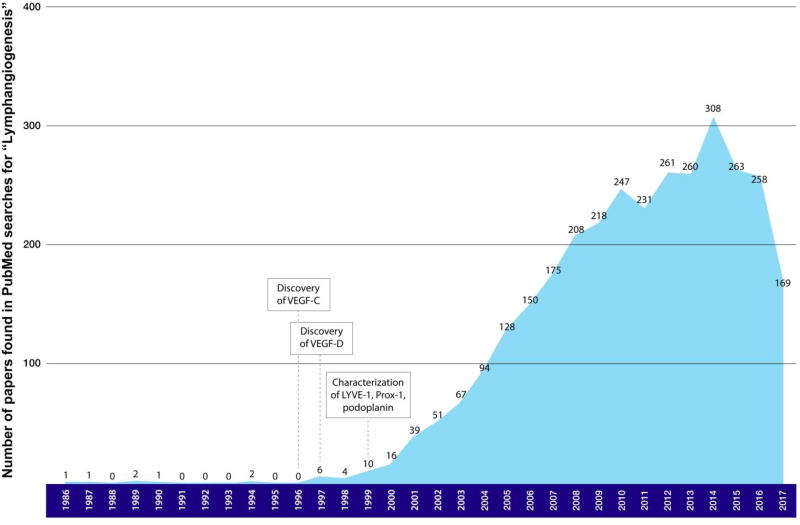
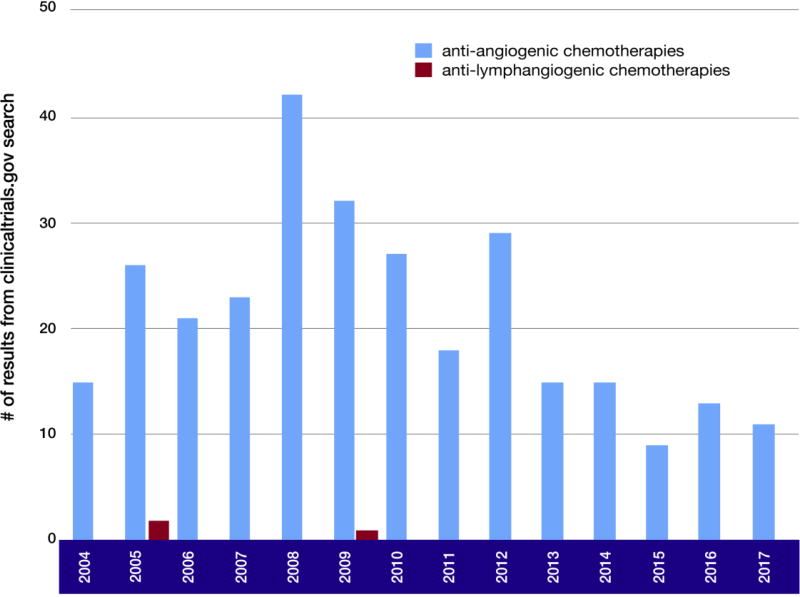
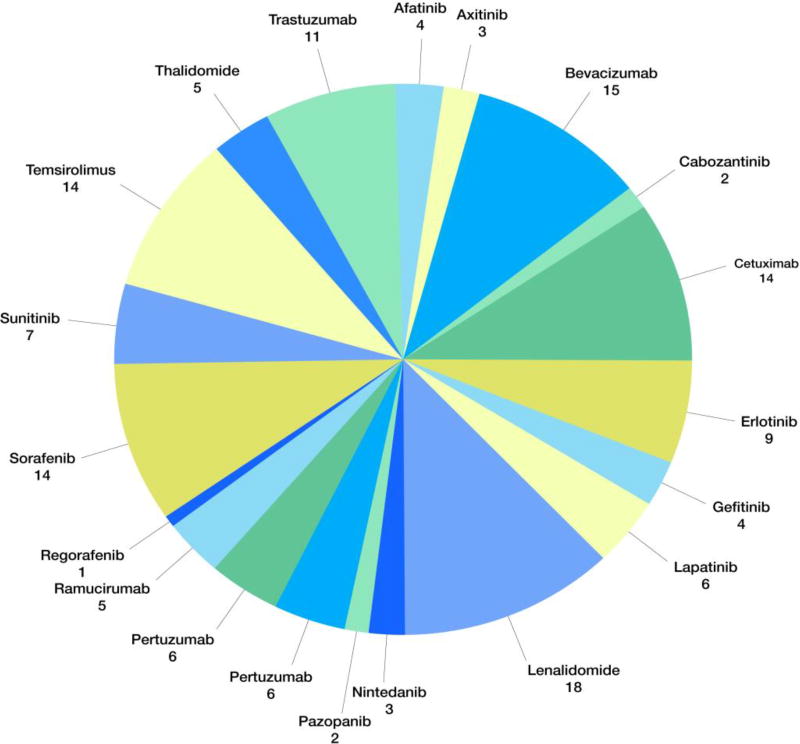
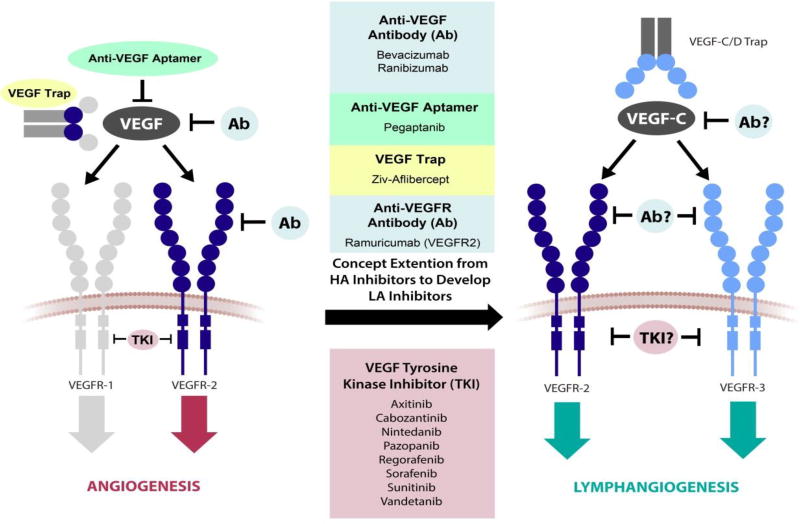
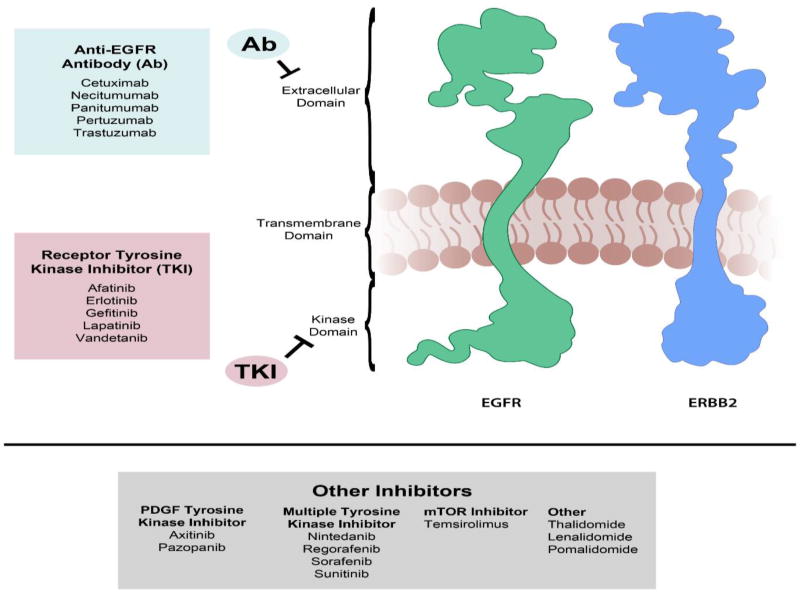
In recent years, lymphangiogenesis, the process of lymphatic vessel formation from existing lymph vessels, has been demonstrated to have a significant role in diverse pathologies, including cancer metastasis, organ graft rejection, and lymphedema. Our understanding of the mechanisms of lymphangiogenesis has advanced on the heels of studies demonstrating vascular endothelial growth factor C as a central pro-lymphangiogenic regulator and others identifying multiple lymphatic endothelial biomarkers. Despite these breakthroughs and a growing appreciation of the signaling events that govern the lymphangiogenic process, there are no FDA-approved drugs that target lymphangiogenesis. In this review, we reflect on the lessons available from the development of antiangiogenic therapies (26 FDA-approved drugs to date), review current lymphangiogenesis research including nanotechnology in therapeutic drug delivery and imaging, and discuss molecules in the lymphangiogenic pathway that are promising therapeutic targets.
Keywords: angiogenesis; lymphangiogenesis.
© 2018 Wiley Periodicals, Inc.
Conflict of interest statement
No conflicts of interest, financial or otherwise, are declared by the authors.
Figures
References
-
- Tammela T, Alitalo K. Lymphangiogenesis: Molecular mechanisms and future promise. Cell. 2010;140(4):460–476. - PubMed
-
- Dieterich LC, Seidel CD, Detmar M. Lymphatic vessels: new targets for the treatment of inflammatory diseases. Angiogenesis. 2014;17(2):359–371. - PubMed
-
- Folkman J. Tumor angiogenesis: therapeutic implications. N Engl J Med. 1971;285(21):1182–1186. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
