

Gaps in Receipt of Clinically Indicated Genetic Counseling After Diagnosis of Breast Cancer
- PMID: 29528794
- PMCID: PMC5908222
- DOI: 10.1200/JCO.2017.76.2369
Gaps in Receipt of Clinically Indicated Genetic Counseling After Diagnosis of Breast Cancer
Abstract
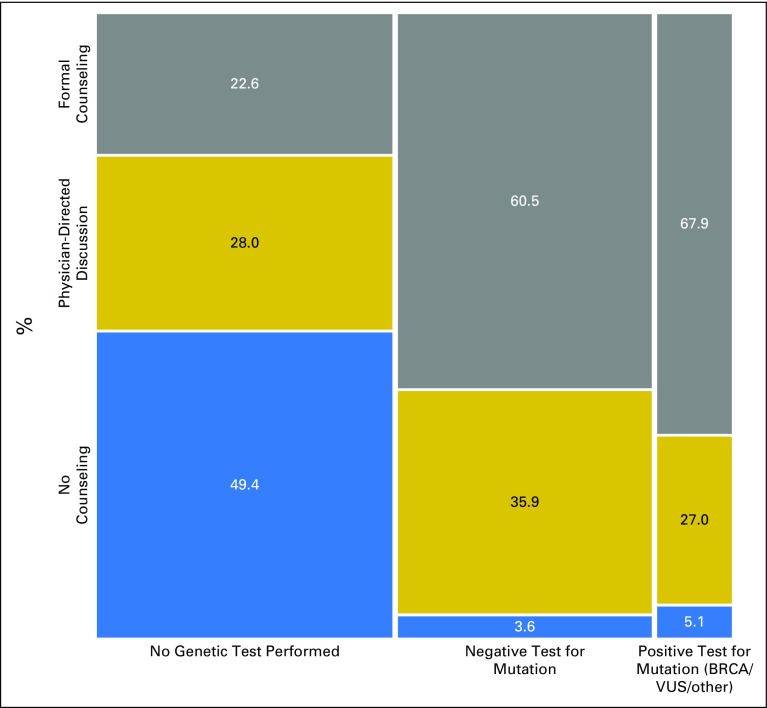
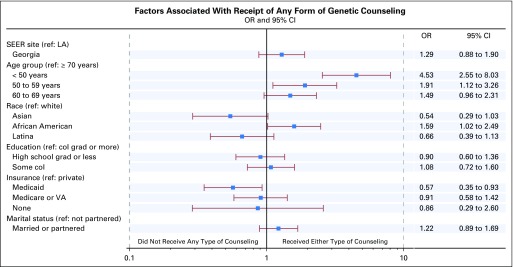
Purpose Little is known about the extent to which genetic counseling is integrated into community practices for patients newly diagnosed with breast cancer. We examined the receipt of clinically indicated genetic counseling in these patients. Patients and Methods We surveyed 5,080 patients between the ages of 20 and 79 years, diagnosed from July 2013 to August 2015 with early-stage breast cancer and reported to the SEER registries of Georgia and Los Angeles County. Surveys were linked to SEER clinical data and genetic test results. The study sample (N = 1,711) comprised patients with indications for formal genetic risk evaluation. Results Overall, 47.4% did not get tested, 40.7% tested negative, 7.4% had a variant of uncertain significance only, and 4.5% had a pathogenic mutation. Three quarters (74.6%) received some form of genetic counseling (43.5%, formal counseling and 31.1%, physician-directed discussion). Virtually all tested patients (96.1%) reported some form of genetic discussion (62.2%, formal counseling and 33.9%, physician-directed discussion). However, only one half (50.6%) of those not tested received any discussion about genetics. Younger women were more likely to report some type of counseling, controlling for other factors: odds ratio, 4.5 (95% CI, 2.6 to 8.0); 1.9 (95% CI, 1.1 to 3.3); and 1.5 (95% CI, 1.0 to 2.3) for women younger than 50 years of age, 50 to 59 years of age, and 60 to 69 years of age versus those 70 years of age and older. Patients' assessments of the amount of information they received about whether to get tested were similarly high whether they were counseled by a genetics expert or by a physician only (80.8% v 79.4% stated information was just right, P = .59). Conclusion Less than one half (43.5%) of patients with clinical indications received formal genetic counseling. There is a large gap between mandates for timely pretest formal genetic counseling in higher-risk patients and the reality of practice today.
Figures
References
-
- Daly MB, Pilarski R, Berry M, et al. NCCN guidelines insights: Genetic/familial high-risk assessment: Breast and ovarian, version 2.2017. J Natl Compr Canc Netw. 2017;15:9–20. - PubMed
-
- Hughes KS: Genetic testing: What problem are we trying to solve? J Clin Oncol 35:3789-3791, 2017. - PubMed
-
- Ahn S, Port ER. Genetic testing in patients with newly diagnosed breast cancer: Room for improvement. J Clin Oncol. 2017;35:2221–2223. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
