

Hospital Variation in Intensive Care Resource Utilization and Mortality in Newly Diagnosed Pediatric Leukemia
- PMID: 29528977
- PMCID: PMC5986594
- DOI: 10.1097/PCC.0000000000001525
Hospital Variation in Intensive Care Resource Utilization and Mortality in Newly Diagnosed Pediatric Leukemia
Abstract
Objectives: To evaluate hospital-level variability in resource utilization and mortality in children with new leukemia who require ICU support, and identify factors associated with variation.
Design: Retrospective cohort study.
Setting: Children's hospitals contributing to the Pediatric Health Information Systems administrative database from 1999 to 2011.
Patients: Inpatients less than 25 years old with newly diagnosed acute lymphocytic leukemia or acute myeloid leukemia requiring ICU support (n = 1,754).
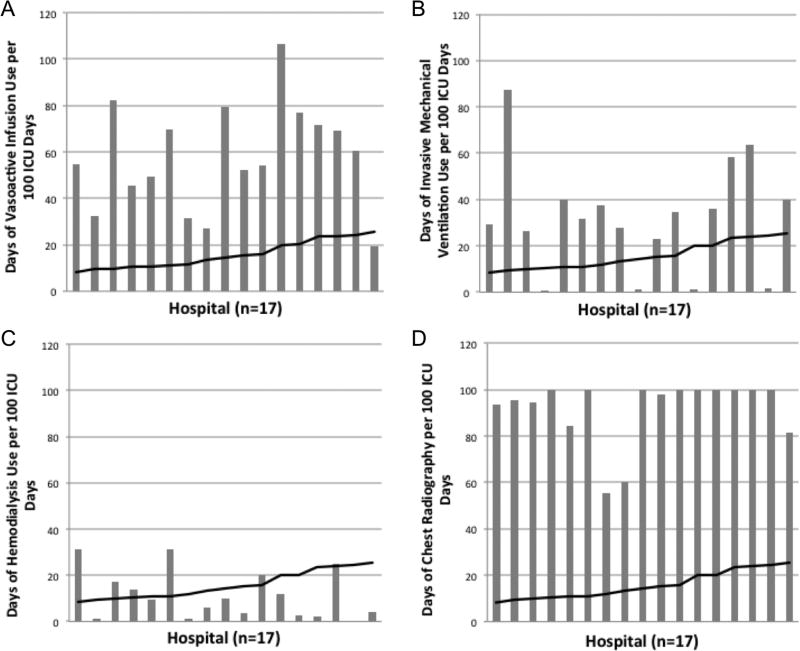
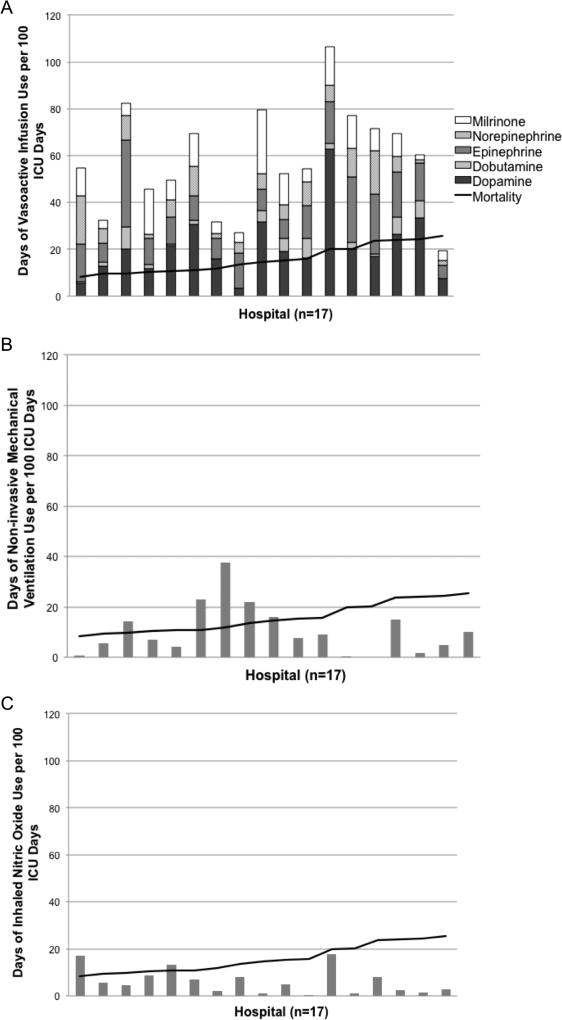
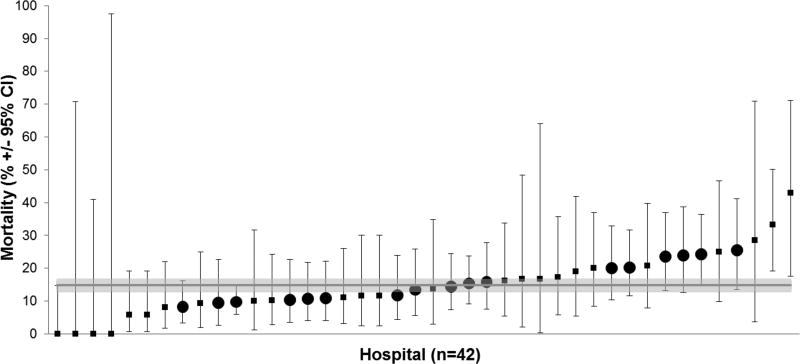
Interventions, measurements, and main results: Evaluated exposures included leukemia type, year of diagnosis, and hospital-wide proportion of patients with public insurance. The main outcome was hospital mortality. Wide variability existed in the ICU resources used across hospitals. Combined acute lymphocytic leukemia and acute myeloid leukemia mortality varied by hospital from 0% (95% CI, 0-14.8%) to 42.9% (95% CI, 17.7-71.1%). A mixed-effects model with a hospital-level random effect suggests significant variation across hospitals in mortality (p = 0.007). When including patient and hospital factors as fixed effects into the model, younger age, acute myeloid leukemia versus acute lymphocytic leukemia diagnosis, leukemia diagnosis prior to 2005, hospital-wide proportion of public insurance patients, and hospital-level proportion of leukemia patients receiving ICU care are significantly associated with mortality. The variation across hospitals remains significant with all patient factors included (p = 0.021) but is no longer significant after adjusting for the hospital-level factors proportion of public insurance and proportion receiving ICU care (p = 0.48).
Conclusions: Wide hospital-level variability in ICU resource utilization and mortality exists in the care of children with leukemia requiring ICU support. Hospital payer mix is associated with some mortality variability. Additional study into how ICU support could be standardized through clinical practice guidelines, impact of payer mix on hospital resources allocation to the ICU, and subsequent impact on patient outcomes is warranted.
Conflict of interest statement
Figures
Comment in
-
Are We the Best We Can Be?Pediatr Crit Care Med. 2018 Jun;19(6):592-593. doi: 10.1097/PCC.0000000000001542. Pediatr Crit Care Med. 2018. PMID: 29863648 No abstract available.
References
-
- Howlader N, Noone AM, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2011. Bethesda, MD: Apr, 2014. based on November 2013 SEER data submission, posted to the SEER web site.
-
- Ward E, DeSantis C, Robbins A, et al. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin. 2014;64(2):83–103. - PubMed
-
- Unguru Y. The successful integration of research and care: how pediatric oncology became the subspecialty in which research defines the standard of care. Pediatr Blood Cancer. 2011;56(7):1019–1025. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
