

Human T-Lymphotropic Virus type 1c subtype proviral loads, chronic lung disease and survival in a prospective cohort of Indigenous Australians
- PMID: 29529032
- PMCID: PMC5874075
- DOI: 10.1371/journal.pntd.0006281
Human T-Lymphotropic Virus type 1c subtype proviral loads, chronic lung disease and survival in a prospective cohort of Indigenous Australians
Abstract
Background: The Human T-Lymphotropic Virus type 1c subtype (HTLV-1c) is highly endemic to central Australia where the most frequent complication of HTLV-1 infection in Indigenous Australians is bronchiectasis. We carried out a prospective study to quantify the prognosis of HTLV-1c infection and chronic lung disease and the risk of death according to the HTLV-1c proviral load (pVL).
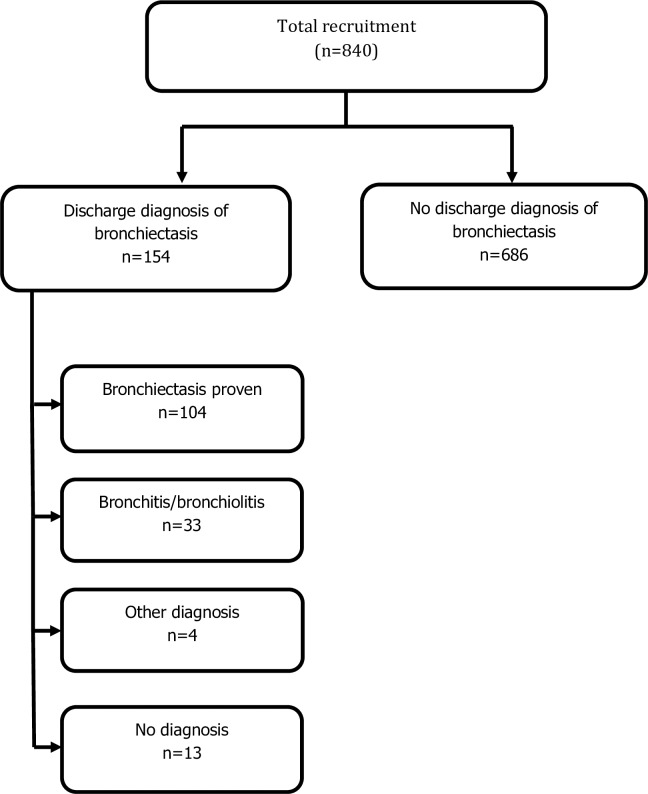
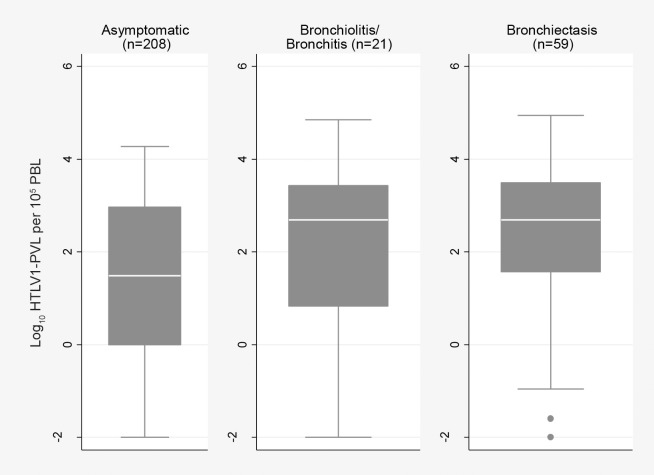
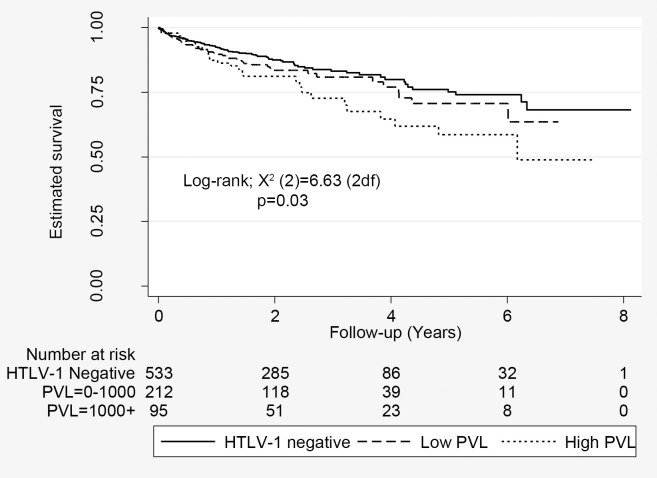
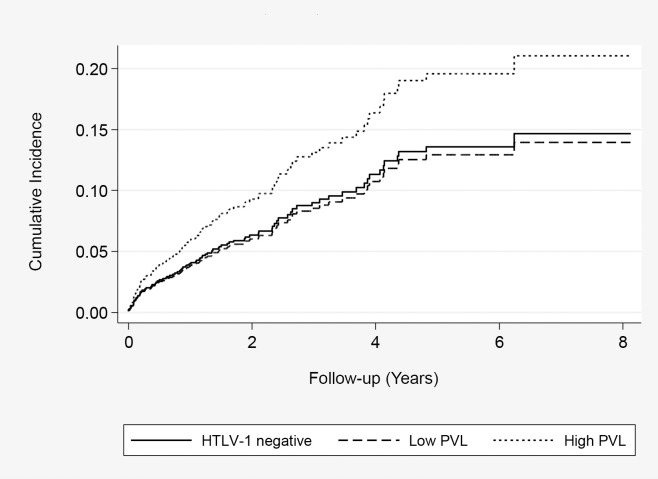
Methodology/principal findings: 840 Indigenous adults (discharge diagnosis of bronchiectasis, 154) were recruited to a hospital-based prospective cohort. Baseline HTLV-1c pVL were determined and the results of chest computed tomography and clinical details reviewed. The odds of an association between HTLV-1 infection and bronchiectasis or bronchitis/bronchiolitis were calculated, and the impact of HTLV-1c pVL on the risk of death was measured. Radiologically defined bronchiectasis and bronchitis/bronchiolitis were significantly more common among HTLV-1-infected subjects (adjusted odds ratio = 2.9; 95% CI, 2.0, 4.3). Median HTLV-1c pVL for subjects with airways inflammation was 16-fold higher than that of asymptomatic subjects. There were 151 deaths during 2,140 person-years of follow-up (maximum follow-up 8.13 years). Mortality rates were higher among subjects with HTLV-1c pVL ≥1000 copies per 105 peripheral blood leukocytes (log-rank χ2 (2df) = 6.63, p = 0.036) compared to those with lower HTLV-1c pVL or uninfected subjects. Excess mortality was largely due to bronchiectasis-related deaths (adjusted HR 4.31; 95% CI, 1.78, 10.42 versus uninfected).
Conclusion/significance: Higher HTLV-1c pVL was strongly associated with radiologically defined airways inflammation and with death due to complications of bronchiectasis. An increased risk of death due to an HTLV-1 associated inflammatory disease has not been demonstrated previously. Our findings indicate that mortality associated with HTLV-1c infection may be higher than has been previously appreciated. Further prospective studies are needed to determine whether these results can be generalized to other HTLV-1 endemic areas.
Conflict of interest statement
The authors declare that no competing interests exist.
Figures
References
-
- Verdonck K, Gonzalez E, Van Dooren S, Vandamme A, Vanham G, et al. (2007) Human T-lymphotropic virus 1: recent knowledge about an ancient infection. Lancet Infect Dis 7: 266–281. doi: 10.1016/S1473-3099(07)70081-6 - DOI - PubMed
-
- Gessain A, Cassar O (2012) Epidemiological aspects and world distribution of HTLV-1 infection. Front Microbiol 3: 388 doi: 10.3389/fmicb.2012.00388 - DOI - PMC - PubMed
-
- Cassar O, Einsiedel L, Afonso PV, A G (2013) HTLV type 1 subtype C molecular variants among Indigenous Australians: New insights on HTLV-1 molecular epidemiology in Australo-Melanesia PLOS Negl Trop Dis 7: e2418 doi: 10.1371/journal.pntd.0002418 - DOI - PMC - PubMed
-
- Einsiedel L, Pham H, Woodman R, Pepperill C, Taylor K (2016) The prevalence and clinical associations of HTLV-1 infection in a remote Indigenous community. Med J Aust 205: 305–309. - PubMed
-
- Einsiedel L, Fernandes L, Spelman T, Steinffort D, Gotuzzo E (2012) Bronchiectasis is associated with Human T-Lymphotropic Virus 1 infection in an Indigenous Australian population. Clin Infect Dis 54: 43–50. doi: 10.1093/cid/cir766 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
