

Physical Functioning Decline and Mortality in Older Adults With Multimorbidity: Joint Modeling of Longitudinal and Survival Data
- PMID: 29529179
- PMCID: PMC6599282
- DOI: 10.1093/gerona/gly038
Physical Functioning Decline and Mortality in Older Adults With Multimorbidity: Joint Modeling of Longitudinal and Survival Data
Abstract
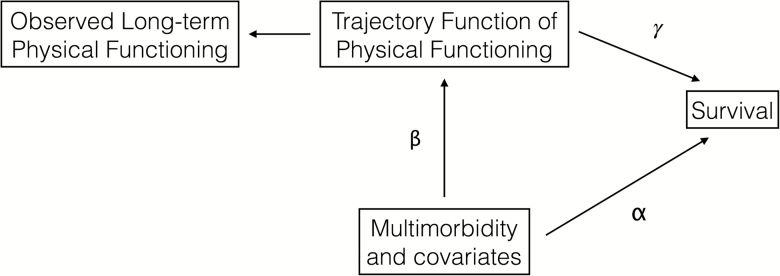
Background: Multimorbidity is common among older adults and strongly associated with physical functioning decline and increased mortality. However, the full spectrum of direct and indirect effects of multimorbidity on physical functioning and survival has not been quantified. We aimed to determine the longitudinal relationship of multimorbidity on physical functioning and quantify the impact of multimorbidity and multimorbidity-attributed changes in physical functioning on mortality risk.
Methods: The Health and Retirement Study (HRS) is a nationally representative population-based prospective cohort of adults aged 51 or older. In 2000, participants were interviewed about physician-diagnosed chronic conditions, from which their multimorbidity-weighted index (MWI) was computed. Between 2000 and 2011, participants reported their current physical functioning using a modified Short Form-36. With MWI as a time-varying exposure, we jointly modeled its associations with physical functioning and survival.
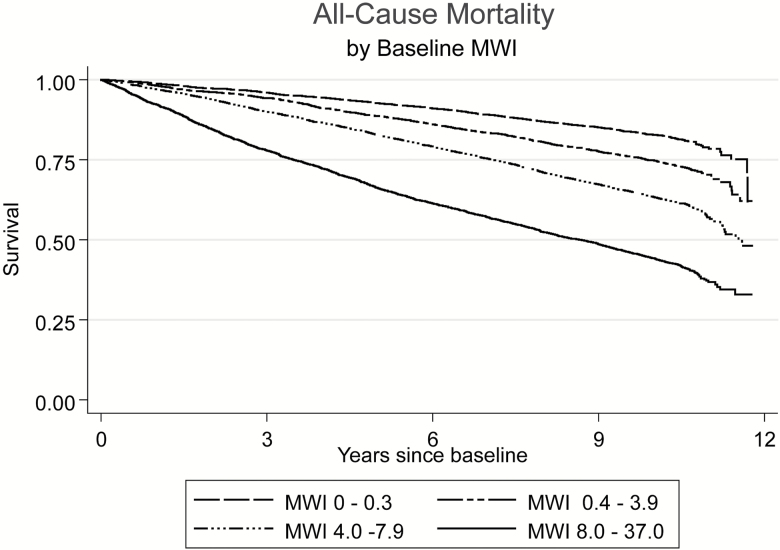
Results: The final sample included 74,037 observations from 18,174 participants. At baseline, participants had a weighted mean MWI of 4.6 ± 4.2 (range 0-36.8). During follow-up, physical functioning declined: -1.72 (95% confidence interval [CI] -1.77, -1.67, p < .001) HRS physical functioning units per point MWI in adjusted models. Over follow-up, 6,362 (34%) participants died. Mortality risk increased 8% (hazard ratio 1.08, 95% CI 1.07-1.08, p < .001) per point MWI in adjusted models. Across all population subgroups, MWI was associated with greater physical functioning decline and mortality risk.
Conclusions: Multimorbidity and its associated decline in physical functioning were significantly associated with increased mortality. These associations can be predicted with an easily interpreted and applied multimorbidity index that can better identify and target adults at increased risk for disability and death.
Figures
References
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373–383. - PubMed
-
- Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
